
 CC-BY 4.0
CC-BY 4.0
Introduction
Hallucinations (perceptions occurring without any external stimuli) and delusions (fixed, false beliefs) are positive symptoms of psychotic disorders, which can lead individuals to lose touch with reality and experience challenges with their thought processes. Studies indicate that these psychotic experiences (PEs) are relatively common in the general population, with a median prevalence of 5-8% (Van Os et al., 2009). Although these experiences may be transient – and can be interpreted positively (Steenhuis et al., 2016) – they indicate a significantly increased risk of developing psychotic disorders later in life (Healy et al., 2019) as well as negative health outcomes, including chronic health conditions, disability and reduced mental well-being (Van Os et al., 2009; Nuevo et al., 2012).
Understanding the risk factors for PEs is therefore important to help identify individuals at higher risk for PEs and potentially inform treatment and prevention strategies. Although there are several known risk factors for PEs – including genetic predispositions, traumatic/adverse childhood experiences, and psychoactive drug use, among numerous others (Van Os et al., 2009; Staines et al., 2022) – here we focus on the role of religion. Religion could influence the risk of PEs, either serving as a protective factor or increasing susceptibility, depending on the nature of the beliefs and type of religiosity. Religion may be a protective factor by offering a sense of community and social support (as social isolation is a risk factor for PEs; Butter et al., 2017; Reininghaus et al., 2008). Conversely, by encouraging a belief in the spiritual/supernatural, religion may foster an increased awareness and perception of alternative sensory experiences, potentially including PEs, increasing their prevalence among religious individuals. Detailed ethnographic work among American Evangelical church-goers suggests that one of the aims of this religious denomination – and potentially religion more broadly – may be for individuals to ‘train’ themselves to become receptive to religious/supernatural phenomena beyond their immediate experience (Luhrmann, 2012). This may, intentionally or not, include unusual sensory experiences (Luhrmann et al., 2010; Luhrmann, 2013) and hence PEs.
Distinguishing religious/spiritual experiences from PEs may be difficult in practice (Johnson & Friedman, 2008; Menezes & Moreira-Almeida, 2010), as they both involve non-material experiences and are inherently subjective. While there is a tension in psychiatry in distinguishing between delusional and religious beliefs, here we broadly follow the American Psychiatric Association’s definition that religious beliefs are not categorised as delusional if they are culturally normative (McKay & Ross, 2021). We also note that while religion may shape the perception of such PEs, this may not necessarily be negative or harmful; hearing voices or hallucinations could be perceived positively if framed in religious terms (e.g., as a sign from God[s], or from deceased friends/family in the afterlife), with religion/spirituality potentially a framework to interpret and cope with said PEs (Johnson & Friedman, 2008; Gearing et al., 2011; Peters et al., 2016).
From the other causal direction, PEs may also shape individuals’ religious beliefs. Psychotic experiences can change one’s identity and worldview (Conneely et al., 2021), including regarding religion (Mohr et al., 2007). This may have public health implications, as several studies have linked religiosity to better health outcomes, including improved mental health (VanderWeele, 2017a, 2017b: although see Halstead et al., 2024; Leurent et al., 2013; Major-Smith et al., 2025a). Understanding the relationship between religious beliefs and psychotic experiences may help inform the development of culturally sensitive mental health interventions and support systems (Koenig, 2009). The interpretation of PEs from a religious perspective may either mitigate or exacerbate distress, depending on individual beliefs and needs. Religious beliefs may impact mental well-being by providing frameworks for understanding and coping with life’s challenges (Luhrmann, 2013), potentially including PEs. These beliefs may serve as protective factors by providing meaning and comfort in difficult times, or, conversely, they could increase risk if they reinforce distressing interpretations of psychotic experiences.
From a theoretical perspective, we may therefore predict a bidirectional causal relationship between PEs and religion. However, previous research in this area is limited in several important ways. While some previous studies have suggested a relationship between religiosity and psychotic experiences (Mohr et al., 2007; Koenig, 2009; Steenhuis et al., 2016; Kovess-Masfety et al., 2018; Huguelet, 2020; Oh et al., 2023), findings across studies have been inconsistent. For instance, a cross-sectional WHO World Mental Health Survey of 25,542 adults over 18 countries found little relationship between religious affiliation or religious service attendance and PEs, yet – among religious individuals specifically – observed a positive relationship for religious beliefs and attitudes (Kovess-Masfety et al., 2018). In contrast, a US sample of college students found a negative association between both Christian religious affiliation and religious importance with PEs (Oh et al., 2023). In addition to this inconsistency, the majority of previous studies were cross-sectional (although see Steenhuis et al., 2016), limiting their ability to establish causality in one direction, let alone potential bidirectional causality. Longitudinal data, with at least three waves of data collection – baseline confounders at time 1, exposure(s) at time 2, and outcome(s) at time 3 – are needed to make stronger claims of causality from observational data (VanderWeele et al., 2016; VanderWeele, 2021).
Additionally, religiosity is a multidimensional concept that encompasses identity, practices, beliefs, values, experiences and motivations (Saroglou, 2011; Pearce et al., 2017). Previous studies have tended to focus on one or two aspects of religiosity (e.g., Oh et al., 2023; Steenhuis et al., 2016) without exploring similarities and differences in religiosity in the same population (for an exception, see Kovess-Masfety et al., 2018). Exploring multiple aspects of religiosity simultaneously may therefore be important, as different aspects of religiosity may have different relationships with PEs. For instance, as attending religious services is often a social activity (Dunbar, 2021), and social activity has a protective association with PEs (Butter et al., 2017), religious service attendance may be a protective factor against developing PEs, even if religious beliefs increase the risk of PEs; on the other hand, in certain religious denominations – such as American Evangelicals – the process of attending to and perceiving religious and supernatural phenomena occurs during church services (Luhrmann, 2012). While there is currently relatively little theoretical work exploring whether and why different aspects of religiosity may vary with PEs, this possibility deserves further empirical exploration, especially given that existing empirical work has found variation in the religiosity-PE relationship by different facets of religiosity (Kovess-Masfety et al., 2018).
Longitudinal studies with repeated PE and religion measures – ideally using a range of religiosity items – are therefore needed to advance this field and provide stronger evidence for potential bidirectional causality between PEs and religion. This is what we aim to do in the present study, using data from the Avon Longitudinal Study of Parents and Children (ALSPAC), which has detailed longitudinal data on both PEs and religion. Using this large-scale, population-based birth cohort in the UK, this study aims to answer the following research questions: i) Do PEs cause subsequent religious beliefs and behaviours? and ii) Do religious beliefs and behaviours cause subsequent PEs? We also focus on a range of religiosity items – including religious belief, identity, attendance and latent classes of religiosity – to assess potential variation in these relationships by different aspects of religiosity.
Methods
ALSPAC Study Description
ALSPAC is a longitudinal birth cohort study which recruited approximately 14,000 pregnant women in the Bristol area of the UK in the early 1990s. These mothers, their children, and their families have been followed for over three decades (for more information on the ALSPAC cohort, see Supplementary Section S1). The present study focuses on PE and religion data from the study offspring in early adulthood (between the ages of 24 and 32 years of age), with additional data from the mothers and partners cohorts used as confounders in analyses. Of the 14,828 offspring alive at 1 year of age who had not withdrawn consent for their data to be used, 5,879 (39.6%) had any data on PEs or religion from adulthood; this is our analytic sample (i.e., the sample we will impute up to and use in analyses; see below). We also note that this ALSPAC sample is predominantly of a White ethnic background (approx. 95%), and – if religious – are mainly Christian, of which the majority identify as Anglican/Church of England (~80%), with smaller numbers of other Christian groups or non-Christian faiths (for more information on the different ALSPAC religious beliefs and affiliations, see Iles-Caven et al., 2023).
Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time. Full details of the ALSPAC consent procedures are available on the study website (https://www.bristol.ac.uk/alspac/researchers/research-ethics/).
Data
Psychotic Experiences
PEs have been assessed in ALSPAC at multiple time-points using Psychosis-Like Symptoms Interviews (PLIKSi) and Questionnaires (PLIKSq) between the ages of 12 and 32 years (Sullivan et al., 2020). For this study we used two sources of PE data: i) PLIKSi data which rated the presence of PEs from ages 12 to 24; and ii) PLIKSq data collected at approximately 32 years of age to assess PEs in the past year. Throughout this paper we refer to these as ‘interview-based PEs’ and ‘questionnaire PEs’, respectively (although we do note that questionnaire data on PEs was self-reported, and hence may be more accurately referred to as ‘psychotic-like experiences’ given the difficulty of knowing whether they meet the criteria for a true psychotic experience).
The semi-structured PLIKSi interview was conducted as part of a wider in-person ALSPAC clinic when study offspring were approximately 24 years of age. This interview included 12 core questions targeting key PEs, such as hallucinations (visual and auditory), delusions (such as being spied on, persecution, thought reading, reference, control, grandiosity, and others), and thought interference (broadcasting, insertion, and withdrawal; see Table S1 for full details of these PEs). Each question began with a structured prompt asking whether participants had experienced any of these symptoms since age 12. If participants responded with “yes” or “maybe” (referred to as “self-reported experiences”), they were further questioned to determine if the experience was psychotic (referred to as “interview-rated experiences”). Experiences were rated as ‘not present’, ‘suspected’, or ‘definitely present’, with PEs attributable to sleep, fever, or substance use excluded. Responses to individual PEs were then combined together to indicate any PEs, with the same categories as above (not present, suspected, or definitely present).
All interviews were conducted in-person by trained psychology graduates and rated according to the Schedule for Clinical Assessment in Neuropsychiatry (SCAN) guidelines. For more information on PLIKSi in ALSPAC, see Sullivan et al. (2020). Of particular relevance for this study, religious experiences deemed as culturally- and/or religiously-normative – e.g., believing that God is communicating with them, or that their will to act was governed by God – were generally not categorised as PEs unless these experiences were interpreted as outside the norms of shared cultural/religious belief (e.g., believing that God has a special mission for them because three red buses drove by in a row would likely be rated as a delusion of reference). Of course, as mentioned above, the boundaries between terms as a ‘normative’ and ‘pathological’ are of course blurry and somewhat open to interpretation (Johnson & Friedman, 2008); however, interviewers were instructed to be conservative in their assessments, and to rate things as ‘non-psychotic’ unless they were confident it met SCAN criteria for a delusion or hallucination.
For the present study, when interview-based PEs were our focal exposure of interest in Research Question 1, we defined PEs as ‘suspected or definite PEs since age 12, not attributable to sleep, fever or substance use’. As sensitivity analyses to explore the impact of different definitions of interview-based PEs on our results, we also used ‘definite PEs since age 12, not attributable to sleep, fever or substance use’. 3,884 participants had data on PEs at age 24 (26.2% of full ALSPAC sample; 66.1% of 5,879 analytic sample).
The self-reported PLIKSq at age 32 comprised eight questions covering a range of PEs, including hallucinations (auditory and visual) and delusions (such as being followed or spied on, persecution, thought reading, reference, control, grandiosity; see Table S2). For each PE, the first question inquired about whether the participant had ever experienced said PE, while the second question asked about its frequency in the past year (if participants gave a positive answer to the first question). These responses were combined together into a binary variable for each PE, denoting either ‘Never/Not in past year’ or ‘Yes, in the past year’. These 8 variables were then combined into a binary variable to indicate ‘any PEs in the past year’; this was our outcome of interest for Research Question 2. 3,956 participants had data on PEs at age 32 (26.7% of full ALSPAC sample; 67.3% of 5,879 analytic sample).
Religiosity
A range of religiosity variables were asked to ALSPAC offspring at approximately 28 years of age (these have been described in detail previously; see Iles-Caven et al., 2019, 2021). For the present study, we focus on four key religiosity variables: i) Religious belief (“Do you believe in God or in some divine power?”, coded as ‘no’, ‘not sure’ or ‘yes’); ii) Religious identity (“What sort of faith/belief would you say you have?”, coded as ‘None’ or ‘Religious’); iii) Religious service attendance (“How often do you attend church/temple/mosque or other religious meetings”, coded as ‘Regular’ [attend minimum once a month] or ‘Occasional/Not at all’ [attend less than once a month]); and iv) religious latent classes (explained in more detail below).
These belief, identity and attendance variables cover a range of theoretically-relevant domains of religiosity (including belief, belonging and behaviour; Saroglou, 2011), and have been used extensively in previous research on religion, both in ALSPAC (Major-Smith et al., 2023; Major-Smith et al., 2025a) and more broadly (McAndrew & Voas, 2011; Li et al., 2016). We also included latent classes of religiosity to provide a variable containing an overall assessment of religiosity (Halstead et al., 2022), which may provide a more granular understanding of relationships between religion and other factors. These latent classes of religiosity were based on a wider range of religion questions (for more details, see Halstead et al., 2022), with four classes identified, broadly described as: “Atheist” (not believe in God), “Agnostic” (not sure if believe in God), “Moderately religious” (believes in God, but rarely attends religious services), and “Highly religious” (believes in God and regularly attends religious services). For religious latent classes, modal class memberships were exported from the latent class analysis and used in subsequent downstream analyses; while we acknowledge that this overlooks the uncertainty inherent in class assignment, relative entropy was high (0.87), indicating good classification accuracy. Depending on the religiosity measure, between 4,098 and 4,453 participants had any religiosity data at age 28 (27.6% to 30.0% of full ALSPAC sample; 69.7% to 75.7% of 5,879 analytic sample).
Confounders
We included a range of potential confounders, which could plausibly cause both the exposures and outcomes of interest, and hence need to be controlled for to estimate an unbiased causal effect (assuming these assumptions regarding confounding are correct and there are no unmeasured confounders). We summarise these confounder variables briefly here, but discuss their measurement and rationale for inclusion as confounders in more detail in Supplementary Section S2. For Research Question 1, as our exposure was PEs since age 12 we predominantly focused on parental confounders measured in pregnancy or shortly afterwards (maternal age, various proxies of socioeconomic position, mother’s marital status, parental adverse childhood experiences, maternal and paternal measures of mental health, and parental religiosity), in addition to some offspring-level confounders measured prior to the exposure (sex assigned at birth, ethnic background, mental health at age 10, locus of control assessed at age 8, and any traumatic/adverse childhood experiences up to age 11). For Research Question 2, as our exposure of interest (offspring religiosity) was assessed at age 28, we used the same core set of confounders as described above, supplemented with additional offspring-level confounders measured in adolescence and early adulthood (mental health at age 24, locus of control at age 16, traumatic adverse childhood experiences up to age 17, various measures of offspring socioeconomic position, relationship status and prior PEs: any differences between confounder sets are noted in Supplementary Section S2).
Data Analyses
Causal Assumptions
Directed Acyclic Graphs (DAGs) of our causal assumptions for Research Questions 1 and 2 can be found in Figures 1A and 1B, respectively. Given these assumptions, conditional on adjusting for said confounders we aim to close all back-door paths and estimate unbiased causal effects for our estimands of interest. These are of course assumptions, and in the Discussion section we return to the plausibility of these assumptions and how violations of them might impact our results (e.g., unmeasured confounding, selection bias, measurement error).
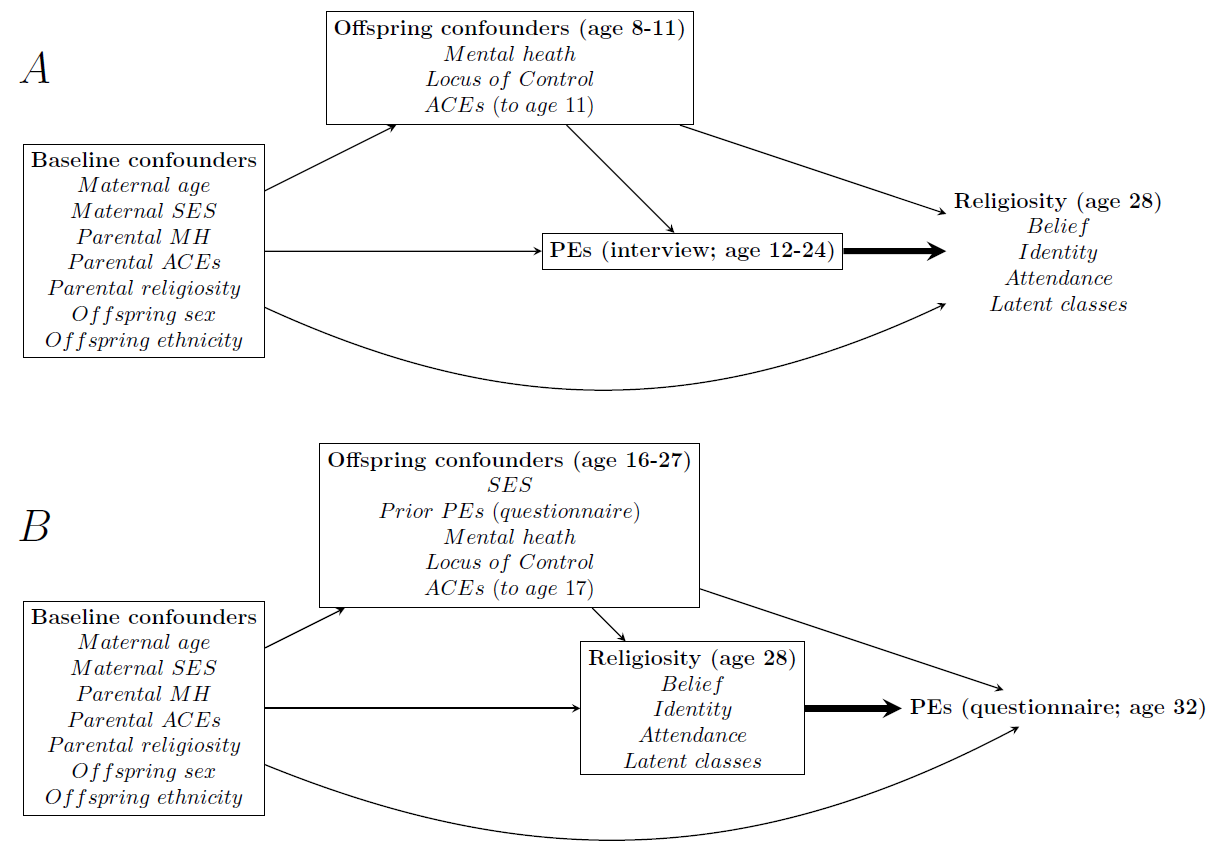
Figure 1 - Directed Acyclic Graphs (DAGs) showing our causal assumptions for both Research Questions 1 (A; upper) and 2 (B; lower). Note that, for simplicity, causal relations between confounding variables within nodes have not been displayed here. Bold arrows denote our causal estimands of interest. SES = Socio-economic status; MH = Mental health; ACEs = Adverse childhood experiences; PEs = Psychotic experiences.
Statistical Analyses
As per our causal models (Figure 1), for Research Question 1 our exposure of interest was ‘suspected or definite PEs since age 12, not attributable to sleep, fever or substance use’ assessed via PLIKSi at age 24, and our outcomes were a range of religiosity measures assessed at age 28 (religious belief, identity, attendance and latent classes). Separate models were used for each outcome, specific to the variable type (i.e., logistic regression for binary outcomes religious identity and attendance; multinomial regression for unordered categorical outcomes religious belief and latent classes). Models were repeated both unadjusted and adjusted, to assess the impact of proposed confounders (see above for details of the confounders in this model).
As it can be difficult to interpret absolute effect sizes from the output of generalised linear models (i.e., odds ratios for logistic models and relative risk ratios for multinomial models) – and to employ formal g-estimation causal inference methods (Hernán & Robins, 2020) for our causal effects of interest – we converted these model results to marginal contrasts in predicted probabilities of the outcome for a change in the exposure (e.g., from ‘no PEs’ to ‘suspected/definite PEs’ being associated with an X%-point increase in the probability of believing in God/a divine power). Briefly, this g-computation/marginal effects approach compares the difference between two counterfactual states of the exposure – e.g., ‘all participants have no PEs’ vs ‘all participants have suspected/definite PEs’ – based on the statistical model and holding all other covariates at their observed values.
As sensitivity analyses to explore the robustness of our models, we repeated the models above using different definitions of ‘PEs at age 24’, using a more stringent definition of interview-based PEs as ‘definite PEs between ages 12-24, not attributable to sleep, fever or substance use’; for this analysis, ‘suspected’ PEs were coded with ‘no PEs’.
For research Question 2, our exposures of interest were the measures of religiosity assessed at age 28 (i.e., religious belief, identity, attendance and latent classes), and our outcome was PEs assessed at age 32 via PLIKSq. Models for each exposure-outcome pair were conducted via logistic regression. As above, models were compared both unadjusted and adjusted for confounders, using g-computation/marginal effects.
Loss-to-follow-up, and hence missing data, is unfortunately common in longitudinal studies, especially in studies using multiple waves of data collection spanning decades, as in the present study. The sample size for complete-case analyses is therefore much smaller than both the full ALSPAC sample (n = 14,828), and our analytic sample (n = 5,879); indeed, complete-case analyses for Research Question 1 have around 1,150 observations, while for RQ2 this drops even further to around 700 observations. Missing data from the full ALSPAC sample to our analytic sample is predominantly due to attrition over time (i.e., participants withdrawing from, or losing contact with, ALSPAC), and hence not having exposure or outcome data: in contrast, missing data within the analytic sample is largely a result of data being aggregated over multiple data collection time-points – 12 for research question 1, 18 for research question 2 – which not all participants with exposure or outcome data took part in (for proportions of missing data for all variables, see Table S3: patterns of missing data across all variables in the analytic sample for research questions 1 and 2 are displayed in Tables S4 and S5). Of those who took part in data collections, relatively few refused to answer the questions on religious beliefs and/or PEs (e.g., <1% of participants who completed the questionnaire with religion questions have missing data for these questions). Based on our assumptions, we believed that our complete-case models would be broadly unbiased. However, to improve power and statistical efficiency we performed multiple imputation by chained equations to impute up to the analytic sample size of 5,879 participants (White et al., 2011; van Buuren, 2018). Unless otherwise stated, all results reported below are based on imputed data. For additional discussion of our assumptions regarding the impact of missing data and our imputation procedure, see Supplementary Section S3.
To explore the level of unmeasured confounding necessary to overturn any observed associations (if present), we also used E-value sensitivity analyses (VanderWeele & Ding, 2017). Briefly, the E-value estimates the level of unmeasured confounding, on the risk ratio scale, necessary to alter an observed association. For instance, an E-value of 2 means that any hypothetical unmeasured confounding would have to double the risk of both the exposure and outcome to make an effect null. While perhaps somewhat difficult to interpret objectively, E-values do provide an assessment of the risk of bias due to unmeasured confounding (although we note that E-values cannot explore potential unmeasured confounding bias away from the null).
Analyses were conducted using Stata version 18, with the ‘margins’ command for g-computation/marginal effects and the ‘mi’ suite of commands for multiple imputation (plus the ‘augment’ option to avoid perfect prediction (White et al., 2010)). As our focus is on causal effect estimation (Hernán & Greenland, 2024), we focus our interpretation on effect estimates and their 95% confidence (or compatibility; Rafi & Greenland, 2020) intervals to provide an indication of the range of plausible effect sizes, as opposed to interpretations based on p-values/statistical significance (Amrhein et al., 2019; McShane et al., 2019).
Results
Descriptive Statistics
Descriptive statistics of all the key PE and religion variables in the full ALSPAC sample, analytic sample and complete case samples are described in Table 1 (descriptive statistics for all variables used in the present study are in Table S3).
Table 1 - Descriptive statistics of psychotic experience (PE) and religion variables used in the present study, comparing the full ALSPAC sample (n = 14,828), the analytic sample used for multiple imputation (i.e., offspring with any PE or religiosity data; n = 5,879; 39.6% of full sample), the complete-case analysis for Research Question 1 (n = 1,158; 7.8% of full sample; 19.7% of analytic sample), and the complete-case analysis for Research Question 2 (n = 712; 4.8% of full sample; 12.1% of analytic sample).
Variable and responses | Full sample (n = 14,828) | Analytic sample (n = 5,879) | Complete-case sample for RQ1 (n = 1,158) | Complete-case sample for RQ2 (n = 712) |
|---|---|---|---|---|
Interview-based PEs from age 12-24 (not attributable to sleep, fever or substance use) | ||||
None | 3,476 (89.5%) | 3,476 (89.5%) | 1,065 (92.0%) | - |
Suspected | 153 (3.9%) | 153 (3.9%) | 32 (2.8%) | - |
Definite | 255 (6.6%) | 255 (6.6%) | 61 (5.3%) | - |
Total | 3,884 | 3,884 | 1,158 | - |
Missing | 10,944 (73.8%) | 1,995 (33.9%) | 0 (0.0%) | - |
Questionnaire-based PEs at age 32 in past year | ||||
No | 3,343 (84.5%) | 3,343 (84.5%) | - | 635 (89.1%) |
Yes | 613 (15.5%) | 613 (15.5%) | - | 77 (10.8%) |
Total | 3,956 | 3,956 | - | 712 |
Missing | 10,872 (73.3%) | 1,923 (32.7%) | - | 0 (0.0%) |
Offspring belief in God/a divine power (age 28) | ||||
No | 2,503 (56.2%) | 2,503 (56.2%) | 654 (556.5%) | 414 (58.2%) |
Not sure | 1,195 (26.8%) | 1,195 (26.8%) | 301 (26.0%) | 179 (25.1%) |
Yes | 755 (17.0%) | 755 (17.0%) | 202 (17.5%) | 119 (16.7%) |
Total | 4,453 | 4,453 | 1,157 | 712 |
Missing | 10,375 (70.0%) | 1,426 (24.3%) | 1 (0.1%) | 0 (0.0%) |
Offspring religious identity (age 28) | ||||
None | 2,890 (65.4%) | 2,890 (65.4%) | 764 (66.3%) | 466 (65.8%) |
Religious | 1,527 (34.6%) | 1,527 (34.6%) | 389 (33.7%) | 242 (34.2%) |
Total | 4,417 | 4,417 | 1,153 | 708 |
Missing | 10,411 (70.2%) | 1,462 (24.9%) | 5 (0.4%) | 4 (0.6%) |
Offspring religious service attendance (age 28) | ||||
Never/Occasionally | 4,213 (95.4%) | 4,213 (95.4%) | 1,084 (94.4%) | 661 (93.6%) |
Regular (min 1/month) | 204 (4.6%) | 204 (4.6%) | 64 (5.6%) | 45 (6.4%) |
Total | 4,417 | 4,417 | 1,148 | 706 |
Missing | 10,411 (70.2%) | 1,462 (24.9%) | 10 (0.9%) | 6 (0.8%) |
Religious latent classes (age 28) | ||||
“Atheist” | 2,473 (60.4%) | 2,473 (60.4%) | 657 (60.2%) | 412 (60.9%) |
“Agnostic” | 878 (21.4%) | 878 (21.4%) | 228 (20.9%) | 141 (20.9%) |
“Moderately religious” | 444 (10.8%) | 444 (10.8%) | 115 (10.5%) | 59 (8.7%) |
“Highly religious” | 303 (7.4%) | 303 (7.4%) | 91 (8.3%) | 64 (9.5%) |
Total | 4,098 | 4,098 | 1,091 | 676 |
Missing | 10,730 (72.4%) | 1,781 (30.3%) | 67 (5.8%) | 36 (5.1%) |
Of participants with interview-based PE data at age 24, 3.9% were suspected as having PEs since age 12, with 6.6% definite cases. At age 32, 15.5% of participants were coded as having experienced questionnaire-based PEs in the past year. Regarding religiosity, the majority of participants did not believe in god/a divine power (56.2%), or identify with a religious affiliation (65.4%), while only a minority of participants regularly attended religious services (4.6%). In terms of the religious latent classes, the majority were classified as “Atheist” (60.4%), with 21.4% as “Agnostic”, 10.8% as “Moderately religious” and only 7.4% as “Highly religious”. Proportions of religiosity were similar in the full, analytic and complete-case samples, although somewhat fewer participants with PEs were in the complete-case samples compared to the full or analytic samples; from 10.5% to 8.0% suspected/definite interview-based PEs at age 24, and from 15.5% to 10.8% questionnaire-based PEs at age 32.
Consistent with previous ALSPAC research (Boyd et al., 2013; Fraser et al., 2013; Cornish et al., 2020; Fernández-Sanlés et al., 2021), there were many differences between the full ALSPAC sample and the analytic sample for a number of variables measured at baseline in pregnancy (Table S3). For instance, mothers in the analytic sample were older (full sample: mean = 27.99 years, SD = 4.97; analytic sample: mean = 29.08, SD = 4.63) and more likely to be educated to degree level (full sample = 12.9%; analytic sample = 18.5%), while study offspring in the analytic sample were more likely to be female (full sample = 49.0%; analytic sample = 62.2%) and from a White ethnic background (full sample = 5.1%; analytic sample = 4.1%).
Research Question 1: Associations between interview-based PEs from age 12-24 years and religiosity at 28 years
Cross-tabulations between the exposure and outcomes suggested a positive relationship between interview-based PEs and later religiosity (Table S6). For instance, based on the imputed datasets, 24.2% of participants with PEs believed in God/a divine power compared to 17.4% of participants without PEs. These results were confirmed in the unadjusted models, with imputed and complete-case results broadly similar (Table S7).
These patterns of results were largely replicated in the adjusted models, with imputed and complete-case results again broadly consistent (Figure 2 and Table S8 for marginal effects; Table S7 for odds/relative risk ratio estimates and E-values).
In these adjusted models, interview-based PEs were associated with an increased probability of answering ‘yes’ to religious belief (relative risk ratio [RRR] = 1.65, 95% confidence/compatibility interval [CI] = 1.15 to 2.38, p = 0.007), with a weaker relationship reported for ‘not sure’ (RRR = 1.29, 95% CI = 0.98 to 1.70, p = 0.074). On the marginal effects scale, this corresponded to a 5.7%-point (95% CI = 0.7% to 10.7%) increase in the probability of answering ‘yes’ (from approximately 17.5% to 23.2%), and a 7.8%-point (95% CI = 1.9% to 13.7%) decrease in the probability of answering ‘no’ (from approximately 55.8% to 48.0%), with smaller differences for ‘not sure’ (a 2.1%-point difference [95% CI = -2.9% to 7.0%]). The E-value necessary to overturn the positive association for ‘yes’ responses, relative to the baseline category of ‘no’, was 1.89 for the point estimate (based on RRR = 1.65]) and 1.35 for the lower 95% CI (based on RRR = 1.15); that is, unmeasured confounding which nearly doubled the risk of the exposure and outcome would be needed to make the result null, while unmeasured confounding which increased the risk of the exposure and outcome by approximately 35% would be needed to make the 95% CI cross the null.
Interview-based PEs were associated with a 30% increase in the odds of reporting a religious identity (odds ratio [OR] = 1.31, 95% CI = 1.01 to 1.69, p = 0.030), corresponding to a 5.6%-point (95% CI = 0.2% to 11.0%) increase in the probability of identifying as religious (from approximately 35.0% to 40.6%). Compared to religious belief, slightly lower levels of unmeasured confounding would be needed to alter these religious identity results (E-value for point estimate = 1.55 [based on OR = 1.31]; E-value for lower 95% CI = 1.08 [based on OR = 1.01]). Due to the smaller number of participants regularly attending religious services, effect sizes were estimated with greater uncertainty but were plausibly null (OR = 1.45, 95% CI = 0.82 to 2.57, p = 0.200), with PEs associated with a 1.7%-point (95% CI = -1.0% to 4.4%) increase in the probability of regular religious service attendance (from approximately 4.9% to 6.5%). The E-value necessary to make the point estimate of religious attendance null was large (E-value = 2.26 [based on OR = 1.45]), but as the lower 95% CI already crossed the null (OR = 0.82), an E-value for the lower 95% CI could not be computed.
For the religious latent classes, with “Atheist” as the reference category, interview-based PEs were associated with a an increased probability of being either “Moderately religious” (RRR = 1.53, 95% CI = 1.05 to 2.23, p = 0.028) or “Highly religious” (RRR = 2.08, 95% CI = 1.28 to 3.36, p = 0.003), but little association with “Agnostic” (RRR = 1.04, 95% CI = 0.75 to 1.42, p = 0.828). On the marginal effects scale, interview-based PEs were associated with a 6.0%-point (95% CI = 0.2% to 11.7%) decrease in the probability of being classified as “Atheist” (from approximately 60.6% to 54.6%), little effect on being classified as “Agnostic” (a 2.0%-point decrease, 95% CI = -6.5% to 2.6%), a 3.4%-point (95% CI = -0.7% to 7.5%) increase in the probability of being classified as “Moderately religious” (from approximately 10.8% to 14.2%), and a 4.5%-point (95% CI = 0.8% to 8.2%) increase in the probability of being classified as “Highly religious” (from approximately 7.1% to 11.6%). E-values were as follows: “Agnostic” (E-value for point estimate = 1.18 [based on RRR = 1.04]; E-value for the lower 95% CI could not be computed as it already crossed the null [based on RRR = 0.75]); “Moderately religious” (E-value for point estimate = 2.43 [based on RRR = 1.53]; E-value for lower 95% CI = 1.28 [based on RRR = 1.05]); “Highly religious” (E-value for point estimate = 3.58 [based on RRR = 2.08]; E-value for lower 95% CI = 1.88 [based on RRR = 1.28]).
Results were comparable for the sensitivity analyses using the more stringent definitions of ‘definite interview-based PEs’ (Tables S9-S11).
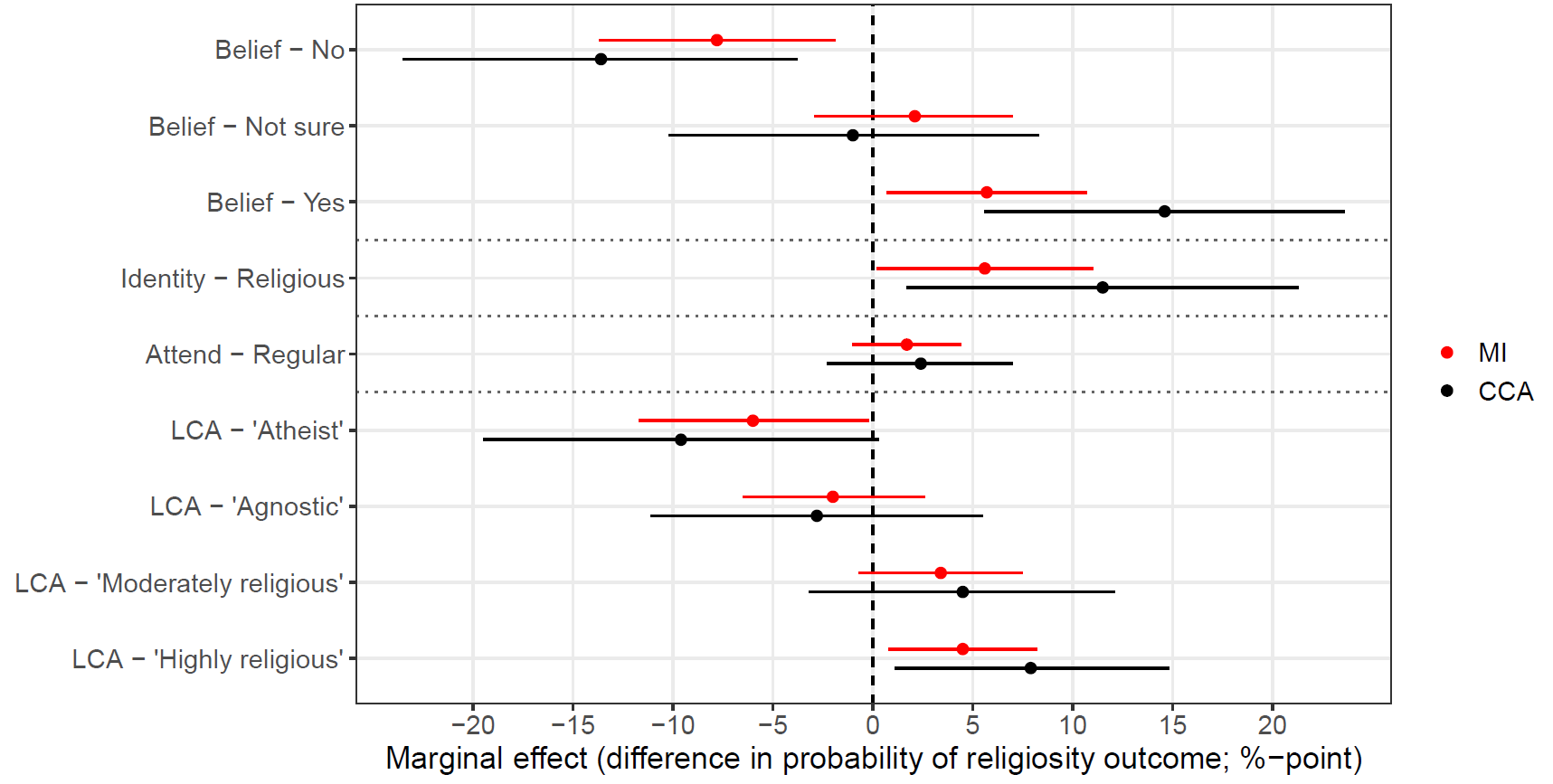
Figure 2 - Results of Research Question 1, with interview-based psychotic experience (PE) exposure ‘any suspected/definite PEs since age 12’ assessed at age 24 and the religiosity outcomes at age 28. Estimates are the marginal effects of a change in the PE exposure (i.e., from ‘none’ to ‘suspected/definite’) on a change in the outcome, based on confounder-adjusted models. For instance, in the multiply imputed results, PEs were associated with an 7.8%-point reduction in the probability of answering ‘no’ to religious belief. Results are displayed for both the complete-case samples (n = 1,091 to 1,157; black) and from multiply imputed datasets (n = 5,879; red). Error bars denote 95% confidence/compatibility intervals. LCA = Latent class analysis; MI = Multiple imputation; CCA = Complete-case analyses.
Research Question 2: Associations between religiosity at 28 years and questionnaire-based PEs at age 32
Cross-tabulations between the exposure and outcomes suggested a positive relationship between religiosity and later questionnaire-based PEs (Table S12). For instance, based on the imputed datasets, 20.4% of participants who believed in God/a divine power had PEs, compared to 13.0% of participants who did not believe, while 21.6% of participants who attended regular religious services had PEs, compared to 15.8% of participants who did not attend regularly. These results were confirmed in the unadjusted models, with imputed and complete-case results again broadly similar (Table S13).
These patterns of results were broadly replicated in the adjusted models, albeit with results for religious identity and attendance attenuated towards the null. Imputed and complete-case results were again largely similar (Figure 3 and Table S14 for marginal effects; Table S13 for odds ratio estimates and E-values).
For the religious belief exposure, participants who answered either ‘not sure’ or ‘yes’ were associated with an increased probability of having questionnaire-based PEs relative to those who answered ‘no’ (Not sure: OR = 1.61, 95% CI = 1.24 to 2.09, p < 0.001; Yes: OR = 1.63, 95% CI = 1.19 to 2.23, p = 0.002). On the marginal effects scale, this model corresponded to a 5.5%-point increase in answering ‘not sure’ (95% CI = 2.4% to 8.6%; from approximately 13.5% to 19.0%) and a 5.7%-point increase in answering ‘yes’ (95% CI = 1.8% to 9.5%; from approximately 13.5% to 19.2%). The E-values for ‘not sure’ responses, relative to the baseline category ‘no’, were 1.85 for the point estimate (based on OR = 1.61) and 1.47 for the lower 95% CI (based on OR = 1.24); the corresponding E-values for ‘yes’ responses were 1.87 for the point estimate (based on OR = 1.63) and 1.41 for the lower 95% CI (based on OR = 1.19).
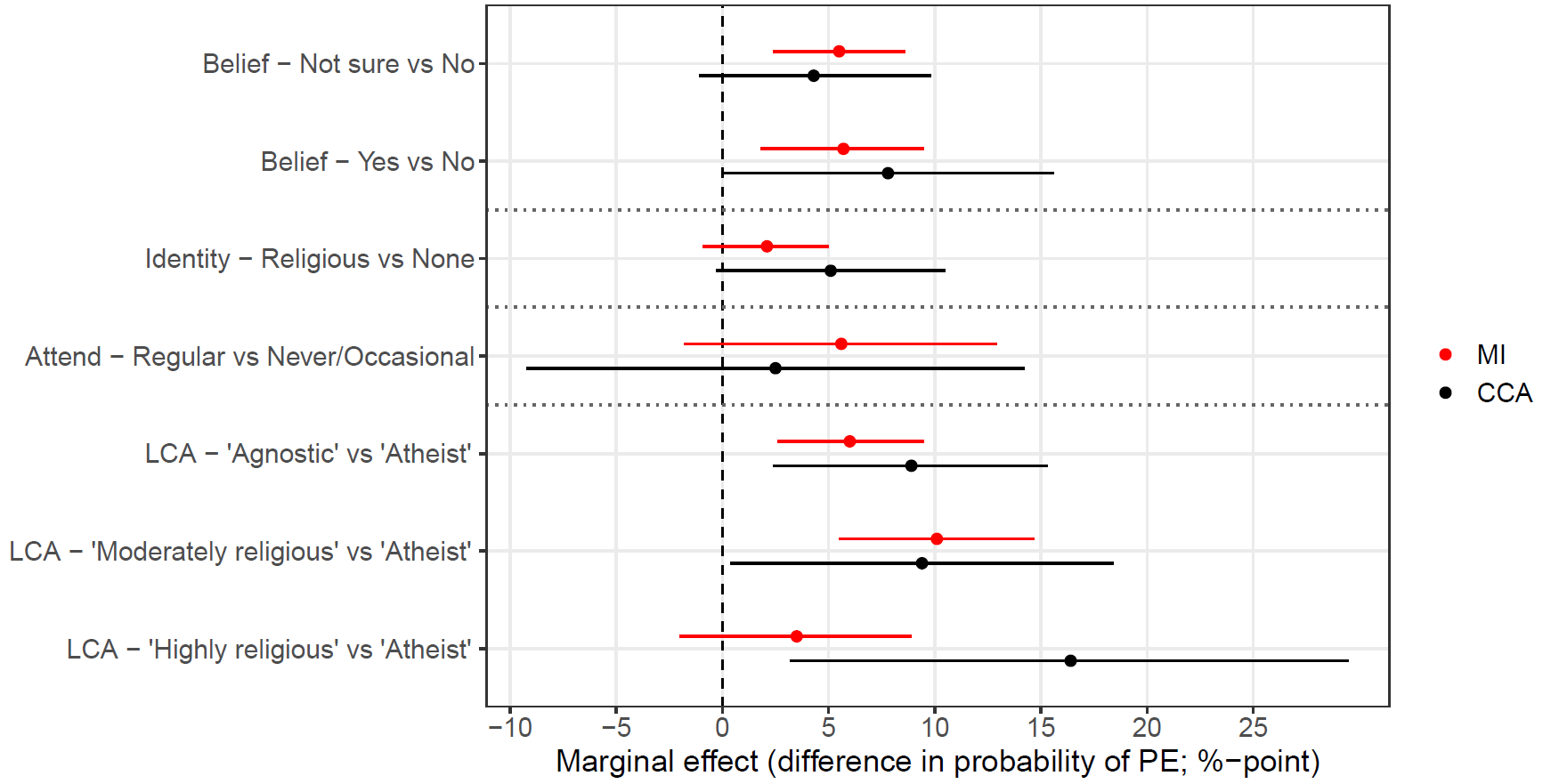
Figure 3 - Results of Research Question 2, with religiosity exposures at age 28 and the questionnaire-based psychotic experience (PE) outcome at age 32. Estimates are the marginal effects of a change in the religiosity exposure (e.g., from ‘no’ to ‘yes’ for religious belief) on a change in the outcome, based on confounder-adjusted models. For instance, in the multiply imputed results, participants who believed in God/a divine power were associated with a 5.7%-point increase in the probability of having PEs. Results are displayed for both the complete-case samples (n = 676 to 712; black) and from multiply imputed datasets (n = 5,879; red). Error bars denote 95% confidence/compatibility intervals. LCA = Latent class analysis; MI = Multiple imputation; CCA = Complete-case analyses.
Weaker effects of religious identity were observed (OR = 1.19, 95% CI = 0.93 to 1.54, p = 0.169), corresponding to a marginal effect of a 2.1%-point increase in questionnaire-based PEs (95% CI = -0.9% to 5.0%; from approximately 15.4% to 17.4%). The E-value for the point estimate was 1.41 (based on OR = 1.19; as lower 95% CI crossed the null, said E-value could not be calculated). Associations with religious attendance were potentially larger but carried greater uncertainty (OR = 1.54, 95% CI = 0.91 to 2.63, p = 0.109), corresponding to a 5.6%-point increase in questionnaire-related PEs with regular religious attendance (95% CI = -1.8% to 12.9%; from approximately 15.8% to 21.4%). The E-value for the point estimate was 1.79 (based on OR = 1.54; as lower 95% CI crossed the null, said E-value could not be calculated). Although somewhat weaker and/or more uncertain compared to religious belief, associations with both religious identity and attendance and questionnaire-based PEs were still predominantly positive.
The latent class results were more nuanced, as, relative to the baseline “Atheist” class, “Agnostic” and “Moderately religious” participants were associated with a greater probability of questionnaire-based PEs (“Agnostic”: OR = 1.69, 95% CI = 1.27 to 2.24, p < 0.001; “Moderately religious”: OR = 2.25, 95% CI = 1.62 to 3.13, p < 0.001), but with a weaker association with “Highly religious” (OR = 1.36, 95% CI = 0.85 to 2.18, p = 0.192). On the marginal effects scale – and again relative to the baseline “Atheist” class – being “Agnostic” was associated with a 6.0%-point increase in the probability of questionnaire-based PEs (95% CI = 2.6% to 9.5%; from approximately 13.3% to 19.4%), being “Moderately religious” was associated with a 10.1%-point increase (95% CI = 5.5% to 14.6%; from approximately 13.3% to 23.4%), while the relationship with “Highly religious” was weaker and plausibly null (3.5%-point increase, 95% CI = -2.0% to 8.9%). E-values were as follows: “Agnostic” (E-value for point estimate = 1.92 [based on OR = 1.69]; E-value for lower 95% CI = 1.51 [based on OR = 1.27]); “Moderately religious” (E-value for point estimate = 2.37 [based on OR = 2.25]; E-value for lower 95% CI = 1.86 [based on OR = 1.62]); “Highly religious” (E-value for point estimate = 1.61 [based on OR = 1.36]; E-value for the lower 95% CI could not be computed as it already crossed the null [based on OR = 0.85]).
Discussion
This study examined the potential bidirectional relationship between psychotic experiences (PEs) and religiosity using longitudinal data from a large UK birth cohort. Even after adjusting for a range of plausible confounders, we found that individuals who had interview-based PEs at age 24 were more likely to be religious at age 28. In the reverse direction, religiosity at age 28 was also associated with a greater probability of questionnaire-based PEs at age 32. Effects in both directions were particularly strong for religious beliefs, with weaker and more inconsistent evidence found regarding religious identity and service attendance.
Comparing our results to those of previous studies is complicated, both by the fact that most previous studies were cross-sectional and because they did not take a causal inference approach, making it difficult to infer the direction of any putative effect (i.e., whether PEs cause religiosity, or vice versa) and to know whether such associations should be interpreted as causal or not. Nonetheless, the weaker association between PEs and religious service attendance is consistent with the results of Kovess-Masfety et al., who also found a stronger relationship between religious beliefs and PEs, but little/no relationship with religious service attendance (Kovess-Masfety et al., 2018). Also, consistent with other work (Steenhuis et al., 2016), we observed a non-linear relationship between religious latent classes and subsequent PEs, with “Agnostic” and “Moderately religious”– but not “Atheist” or “Highly religious” – individuals at greater risk of later PEs. Our results are, however, inconsistent with other studies, such as those suggesting that a Christian religious affiliation and religious importance were associated with lower rates of PEs (Oh et al., 2023).
Our results suggest that PEs may impact religious beliefs, while religious beliefs may also impact PEs. The interpretation of these patterns, however, is unclear, and many possibilities are plausible. For instance, by changing people’s perceptions and attitudes, PEs may facilitate the adoption of religious beliefs; perhaps comparable to how religious rituals and ceremonies associated with altered conscious states may help develop and strengthen individuals’ religious convictions (De Rios & Winkelman, 1989; Price‐Williams & Hughes, 1994; Lee et al., 2016). In the opposite direction, the interpretative frameworks provided by religious beliefs may amplify or validate unusual experiences, increasing their likelihood of being attended to (Luhrmann et al., 2010; Luhrmann, 2012). Our findings therefore align with previous research suggesting that religious beliefs might provide a framework for individuals for interpreting or coping with psychotic experiences (Luhrmann, 2013; Huguelet, 2020).
More generally, our results suggest a potential positive feedback loop between PEs and religiosity, and highlight the importance of culture and one’s beliefs in the interpretation of said PEs (Luhrmann, 2011; Luhrmann et al., 2015a). One mechanism by which this process may work is by both religion and PEs making individuals more cognitively ‘porous’ – that is, believing the boundary between ‘the mind’ and ‘the outside world’ is more permeable – which has been associated with religious/supernatural experiences (Luhrmann et al., 2021). Regardless of the mechanisms, this potential bidirectional causation between PEs and religiosity has clear practical/methodological implications; namely, future work exploring this relationship from a causal standpoint must take a longitudinal approach, else it may simply not be possible to make any assessment of causality from cross-sectional data as causal effects in both directions are possible (VanderWeele et al., 2016).
These results also suggest differences between religious beliefs and religious service attendance, and their relationship with PEs. Although aspects of religion are highly-correlated, they are not synonymous – many more people claim to have a religious identity than believe in God or regularly attend a place of worship, for example – and our results suggest that the possible bidirectional relationship between religiosity and PEs may be stronger for religious belief than for regular service attendance. One potential, and tentative, interpretation of this is that religious beliefs and PEs are individual-level cognitive factors regarding attitudes and attributions, and so may be more tightly coupled. In contrast, religious behaviours may be more influenced by social factors (e.g., building and maintaining social networks; Dunbar, 2021), and hence have a weaker relationship with PEs. An additional – and not necessarily mutually-exclusive – interpretation is that perhaps the social nature of religious communities acts as a protective factor against the development of PEs among religious individuals (Butter et al., 2017), hence weaking any relationship between PEs and religious attendance. These interpretations are of course very speculative, and additional research is needed to see whether these broad findings replicate before theorising in more depth about potential mechanisms for these differences.
Finally, from a practical perspective, while our results are of course far too preliminary to help inform clinical practice, they do suggest that understanding how religious beliefs influence the development, perception and progression of psychotic symptoms could be valuable, for instance in the development of culturally sensitive mental health interventions and support systems (Koenig, 2009; Huguelet, 2020). Given the known negative outcomes of those with PEs (Van Os et al., 2009), understanding whether religion may moderate or mediate the development of psychotic experiences may be a useful avenue for future work, and ultimately shape efforts to improve mental health outcomes.
Strengths and Limitations
This study possesses key strengths over previous research in this area, namely the use of longitudinal data to explore these relationships in both directions. Other strengths include: i) the use of a range of religiosity measures, to explore variation by different aspects of religiosity; ii) our use of causal inference methods, making our causal estimands clear, in addition to the assumptions required for a causal interpretation to be valid; iii) inclusion of a wide range of plausible confounders to try and remove the threat of unmeasured confounding and reverse causality, as well as E-value sensitivity analyses to explore the levels of unmeasured confounding necessary to alter results; and iv) use of data from a large-scale population-based study, which was broadly representative of the target population at enrolment (Fraser et al., 2013).
Despite these strengths, this study of course possesses some key limitations, regarding both threats to a causal interpretation and conceptual issues regarding the interpretation and generalisability of results. We discuss these in turn, and suggest ways in which future research can build upon and improve our work. A first key threat to causality is unmeasured confounding. While we endeavoured to include all relevant confounders necessary to block all biasing back-door paths, this is never possible to conclusively prove from observational data. While it is impossible to know the true level of unmeasured confounding (if any), our E-value sensitivity analyses suggested that many results were robust to some degree of unmeasured confounding. For instance, for Research Question 1 and the religious belief outcome (Table S5), unmeasured confounding would have to increase the risk of both the exposure and outcome by approximately 35% to make the 95% CIs cross the null. As the inclusion of measured confounders did not appear to greatly alter the observed relationships, this may suggest that the inclusion of additional confounders would similarly have relatively little impact on results. We of course note that this is a strong assumption, and one which may be incorrect if important confounders were overlooked. For instance, traits we were not able to control for – such as the ability to suspend or ignore the need for scientific/empirical evidence when forming or maintaining beliefs, or analytic cognitive style (Ross et al., 2017) – could be a common cause of both religiosity and PEs.
A further threat to causality is measurement error, which also links to limitations regarding our measured constructs. There are many sources of measurement error which could result in bias. Although common in the literature, our reliance on rather crude proxies for potentially-complex religious constructs could mean that we are not fully capturing aspects of religiosity relevant to PEs, such as the specific aspects of the religious beliefs relevant to understanding and interpreting PEs. For instance, previous theoretical and empirical research has also implicated the role of prayer (Luhrmann et al., 2010, 2013), costly religious rituals (Lee et al., 2016), and the extent to which religious beliefs are ‘personal’ rather than ‘general’ (Van Leeuwen & van Elk, 2019), in altering one’s beliefs and perceptions. Regarding our PE measures, PLIKSi at age 24 was conducted by trained interviewees, so any bias in this measure ought to be minimal, especially regarding coding of religious experiences which may shade into PEs (hearing God, etc.). This nuance may be lost in the self-reported PLIKSq at age 32, potentially leading to conflation of religious and psychotic experiences in some participants, especially as it may often be difficult – if not sometimes impossible – to distinguish between PEs and religious/spiritual experiences (Johnson & Friedman, 2008; Huguelet, 2020); for instance, a recent meta-analysis found that a common category of delusions among adults with psychosis is ‘religious delusions’ (Pappa et al., 2025). If this conflation occurred, this would likely result in a biased positive relationship in Research Question 2 between religiosity and PE outcomes. To help minimise such bias, we therefore highly recommend that future work in this area use interview-based methods to elicit PEs, rather than self-report methods, where possible. Regarding PE measurement, we also acknowledge that grouping together PE symptoms may overlook the possibility that some PE symptoms may have a stronger relationship with religiosity than others (and vice versa). For instance, visual and auditory hallucinations may be more amenable to a religious interpretation than paranoid symptoms of delusions of persecution. We hope that other future studies follow up on this area, exploring both PEs and religiosity in more depth and granularity. We also note that measurement error in our confounders – especially for hard-to-measure social and psychological constructs such as socioeconomic position, locus of control and religiosity – may also lead to bias, as confounding back-door paths may not be fully blocked (i.e., residual confounding; Greenland, 1980).
A more conceptual limitation – and a key area for future research – is to understand how PEs may impact religiosity (and vice versa). That is, what are the specific mechanisms by which PEs result in a change in religious beliefs (again, and vice versa)? More information about the content of people’s PEs and their religious beliefs/experiences, and how they interpret these, is therefore needed. For example, are voices/visions from PEs seen as positive, negative, or neutral (Steenhuis et al., 2016)? What are the content of people’s religious beliefs (Van Leeuwen & van Elk, 2019)? Do religion and PEs alter how ‘porous’ peoples’ minds are to experiencing unusual and/or psychotic-like experiences (Luhrmann et al., 2021)? What is the role of prayer in this process (Luhrmann et al., 2010)? What is the role of ‘spirituality’, as opposed to formal religion, in these relationships? How do the cultural and religious traditions in which one lives alter this relationship (Luhrmann, 2012; Luhrmann et al., 2015a)? Probing these factors in more depth, including through the use of in-depth qualitative interviews and ethnographic approaches, may help us better understand the relationship between religion and PEs, and how and why they may impact different people in different ways.
A final limitation concerns generalisability. ALSPAC is small slice of human variation, mainly White, British, middle-class, largely non-religious (and, if religious, predominantly Christian [and, if Christian, predominantly Anglican/Church of England]). The extent to which results would generalise to other countries, cultures or religious traditions is therefore unclear, especially given how variable interpretation of PEs and supernatural/religious experiences are by culture and religion (Luhrmann, 2011; Luhrmann et al., 2015a; b, 2024), and even between different Christian denominations (Luhrmann, 2012). Despite these open questions regarding generalisability, and reasons for cross-cultural variability in these relationships, we hope that the results of the present study can act as a platform on which further research in this area can build.
Conclusion
Despite these caveats and limitations, we believe that these results are – at present – the best available observational evidence exploring bidirectional causality between PEs and religiosity. While of course still rather limited, we hope that future work will investigate whether these findings replicate and the extent to which they are generalisable across cultures and populations, in addition to probing potential mechanisms in more depth. As well as contributing to theory regarding the relationship between PEs and religiosity, our results may also have downstream practical implications for public health by informing the development of culturally sensitive mental health interventions and support systems, which can also be further explored in future work.
Acknowledgements
We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists, and nurses. Preprint version 3 of this article has been peer-reviewed and recommended by Peer Community In Psychology (https://doi.org/10.24072/pci.psych.100003; Howard, 2025).
Funding
The UK Medical Research Council and Wellcome Trust (Grant ref: 217065/Z/19/Z) and the University of Bristol currently provide core support for ALSPAC. This publication is the work of the authors and Daniel Major-Smith will serve as guarantor for the contents of this paper. A comprehensive list of grants funding is available on the study website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf). This project was made possible through the support of a grant from the John Templeton Foundation (ref no. 61917). The opinions expressed in this publication are those of the author(s) and do not necessarily reflect the views of the John Templeton Foundation. Daniel Major-Smith was also supported by a grant from the Templeton Religion Trust (ref no. TRT-2022-31107). Hannah J Jones is supported by the National Institute for Health and Care Research (NIHR) Bristol Biomedical Research Centre (BRC; grant number: NIHR 203315). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Conflict of interest disclosure
The authors declare that they comply with the PCI rule of having no financial conflicts of interest in relation to the content of the article. The authors declare the following non-financial conflict of interest: Daniel Major-Smith is a recommender for PCI Registered Reports.
Data, scripts, code, and supplementary information availability
ALSPAC data access is through a system of managed open access. Information about access to ALSPAC data is given on the ALSPAC website (http://www.bristol.ac.uk/alspac/researchers/access/) and in the ALSPAC data management plan (http://www.bristol.ac.uk/alspac/researchers/data-access/documents/alspac-data-management-plan.pdf). Data used for this submission will be made available on request to the Executive (alspac-exec@bristol.ac.uk). The datasets presented in this article are linked to ALSPAC project number B4572, please quote this project number during your application.
Analysis code and synthetic ALSPAC datasets (created using the ‘synthpop’ R package; Nowok et al., 2017) are openly-available on DM-S’s GitHub page: https://github.com/djsmith-90/AnalysisCode_PLIKS_RSBB_B4562 (repository archived with DOI in Zenodo here: https://doi.org/10.5281/zenodo.17285482; Major-Smith, 2025). As raw ALSPAC data cannot be released, these synthesised datasets are modelled on the original data, thus maintaining variable distributions and relations among variables (albeit not perfectly), while at the same time preserving participant anonymity and confidentiality, thus allowing this research to be ‘quasi-reproducible’ (Major-Smith et al., 2024). Please note that while these synthetic datasets can be used to follow the analysis scripts, as data are simulated they should not be used for research purposes; only the actual, observed, ALSPAC data should be used for formal research and analyses reported in published work.
The Supplementary Information file associated with this submission is available on the OSF project page (file “PEandReligion_SI_forPCJ.pdf”: https://doi.org/10.17605/OSF.IO/8FJ3B; Major-Smith et al., 2025b).