
 CC-BY 4.0
CC-BY 4.0
Introduction
Huntington’s disease (HD) is defined as a rare and inherited neurodegenerative disease that appears between 30 and 40 years. It is caused by an abnormal cytosine-adenine-guanine trinucleotide expansion within the huntingtin gene on chromosome 4 (McColgan & Tabrizi, 2018). HD particularly affects medium spiny neurons of the striatum that cause progressive motor, cognitive, and psychiatric symptoms. Motor symptoms evolve independently of cognitive and psychiatric disorders that sometimes appear earlier (McAllister et al., 2021).
Motor symptoms enable the clinical diagnosis of HD. They can be split into two distinct and successive phases: hyperkinetic phase and hypokinetic phase (Stoker et al., 2022). Chorea, walking, and balance impairments are encompassed in these symptoms (Berardelli et al., 1999; Vuong et al., 2018). Cognitive disorders refer to psychomotor speed, executive functions (EF), memory, emotion processing, and social cognition (Ho et al., 2003; Snowden, 2017). These disorders usually appear at an early stage of the disease and are associated with dysfunction of the loops connecting the striatum and the frontal lobe (Ho et al., 2003). Later, cognitive disorders extend to language and visuospatial abilities (Snowden, 2017). In addition, studies have shown a positive correlation between EF and walking or balance (Iersel et al., 2008; Ijmker & Lamoth, 2012; Kearney et al., 2013). This highlights the interest to focus on these functions. Still, psychiatric disorders are part of HD (depression, apathy, irritability, anxiety) (Craufurd et al., 2001; Snowden, 2017). These difficulties have a detrimental effect on daily activities and, thus, on autonomy and quality of life (QoL) (Zielonka et al., 2018).
In the absence of curative treatment for the neurodegenerative diseases, studies on the feasibility and relevance of cognitive and motor exercises to delay the onset and progression of symptoms are emerging. Although HD can be detected before the onset of symptoms, few studies have focused on motor-cognitive training in prodromal and manifest HD for secondary and tertiary prevention. Nevertheless, a systematic review concludes that combining motor and cognitive training leads to more consequent effects on cognition, quality of life, and well-being in HD patients (Huynh et al., 2022). Other meta-analyses highlight the positive effects of motor-cognitive training on cognitive and physical functions in older adults with/without cognitive impairments (Gavelin et al., 2021), stroke survivors (Embrechts et al., 2023), and people with Parkinson’s disease (Johansson et al., 2023). However, there is not a clear superiority on motor or cognitive trainings only (Gavelin et al., 2021; Embrechts et al., 2023). The onset of the symptomatic triad of HD is associated with the involvement of a unique subcortical structure, the striatum. This focal point in the brain strengthens the idea of synergical and reciprocal influence of motor and cognitive training in improving clinical symptoms. In fact, these trainings promote structural and functional neuroplasticity in the striatal region and in cortex areas that are linked (i.e. frontosubcortical circuits) (Hamzei et al., 2012; Marusic et al., 2018). Thus, motor-cognitive training could yield additive, synergistic effects on neuroplasticity and potentially help to sustain these benefits (Fissler et al., 2013).
Fabian Herold and other researchers have proposed a classification of motor-cognitive training. While it can be done sequentially (SEQ) on the same day or on different days, the authors distinguish two simultaneous motor-cognitive trainings (Herold et al., 2018). On the one hand, the cognitive task is “additional” to the motor task. The two stimulations are performed independently, and the results of one exercise do not influence the execution of the other (e.g., performing verbal fluency orally while doing squats). This method is known as “dual-task training” (DT). On the other hand, the cognitive task is “incorporated” into the motor task, exercises complement each other and lead to a common goal (e.g., categorizing words into two groups by performing sidesteps to the left or right). This approach is designated as “synergical training” (SYN). It is important to distinguish the two forms of training. While SEQ exercises are performed one after the other, SYN exercises exhibit complementarity between a cognitive task and a motor task. The success of the cognitive task is linked to the success of the associated motor task. Therefore, these exercises are distinct from DT motor-cognitive exercises which involve performing independent cognitive and motor tasks simultaneously (Herold et al., 2018). Although more comparative studies are needed to draw firm conclusions, SEQ training appears to be less effective than simultaneous motor-cognitive trainings (DT or SYN) because the optimal order and the temporal interval between motor and cognitive exercises are not clearly defined. Moreover, simultaneous motor-cognitive trainings are time-efficient approaches. Among these approaches, SYN training is expected to be superior to DT training in promoting neuroplastic effects as the corresponding exercises are closer to daily-life situations and do not induce any priorization effect between the motor and the cognitive tasks (Herold et al., 2018).
The use of exergaming (i.e., interactive video-games that require participants to be physically active to play) as a support for training (Pirovano et al., 2016) is well tolerated in various populations. A previous study has shown that the feasibility and usability of an exergame-based motor-cognitive training are acceptable for older adults with neurocognitive disorders (Manser et al., 2023). Additionally, a systematic review in Parkinson’s disease patients has shown that practicing exergaming is feasible with positive level of motivation, facilitating training adherence and success (Barry et al., 2014). Exergame-based training also appears promising to decrease cognitive, motor, and depressive symptoms in older adults (Van Diest et al., 2013; Yen & Chiu, 2021). Moreover, the use of exergaming - in the context of rehabilitation - seems superior to conventional physiotherapy for improving QoL in people with Parkinson’s disease (Elena et al., 2021). Exergaming is particularly relevant due to the numerous possibilities it offers to combine physical exercises (strength, balance, aerobic) with cognitive exercises, thus forming varied motor-cognitive training sessions (SEQ, SYN, or DT). However, future studies on HD are needed to highlight the superiority of exergaming compared to conventional physical and/or cognitive trainings (Torre & Temprado, 2022).
These observations have supported and guided the development of our exploratory project. Our aim is to investigate the feasibility and acceptability of two exergame-based motor-cognitive trainings in patients with HD. We hypothesize that those programs will be well tolerated by patients with high rates of adherence, few instances of dropouts, and good perceptions about the usefulness, the stimulation, the security, and appropriateness of the programs. Our second aim is to evaluate the preliminary effectiveness of those programs on motor, cognitive, and psychiatric symptoms in patients with HD. We hypothesize that both trainings will improve physical and cognitive functions and QoL as well as decrease psychiatric symptoms. This will be verified using standardized conventional cognitive, physical tests and with validated questionnaires for psychiatric symptoms and QoL. We also suppose that improvements will sustain 3 months after the end of the intervention. Finally, we expect that SYN training will yield more significant improvements on physical, cognitive, and psychiatric symptoms as well as on QoL than SEQ training.
Materials and methods
Study design
This study is a parallel randomized trial that compares two types of exergame-based motor-cognitive training for their feasibility and preliminary effectiveness. Digital support, particularly exergaming, is the preferred method for displaying combined exercises and facilitates the administration and monitoring of care. This exploratory study will be helpful to define the preferred program (synergical or sequential program) for a subsequent larger-scale trial comparing training motor-cognitive with an exergame versus standard care. The study overview is presented in Figure 1.
Participant recruitment, screening, and enrolment
Patients with HD are recruited from the national reference centre for neurogenetic diseases (CNRMN, Centre National de Référence des Maladies Neurogénétiques) at the University Hospital Centre (CHU) of Angers (France). Participation in the study is offered to HD patients attending day hospitalization as part of their routine disease management.
Eligible patients are identified from the active patient list maintained by the CNRMN using their medical records. Patients meeting the pre-defined selection criteria are contacted by phone to introduce the study and to schedule an inclusion visit during their next routine visit to the CNRMN.
During the inclusion visit, if the patient meets the study’s selection criteria (see Table 1) and expresses interest in participating, the principal investigator provides him with both oral and written information (a written information letter in a language understandable to the subject) and addresses any questions he may have. If the patient agrees to participate, the informed consent form is signed in duplicate by all parties involved.
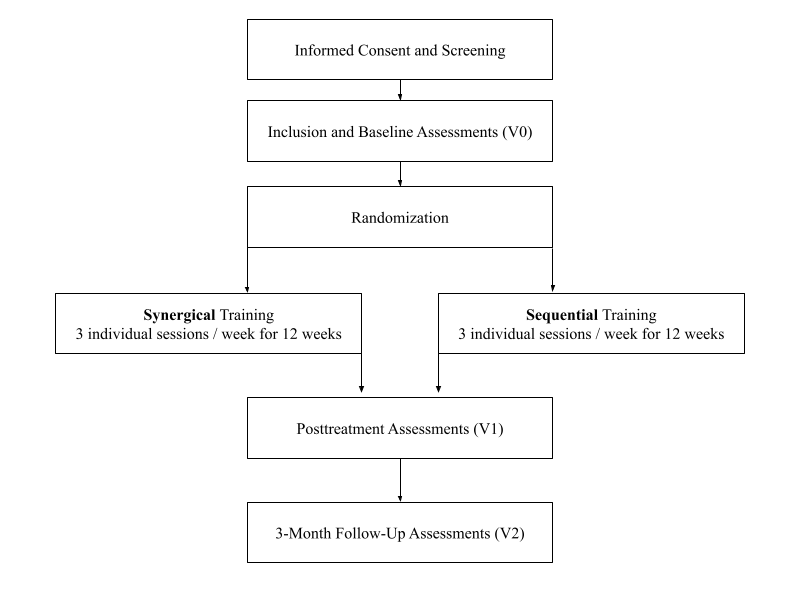
Figure 1 - Flowchart of the study protocol
Table 1 - Inclusion and exclusion criteria
INCLUSION CRITERIA | EXCLUSION CRITERIA |
|---|---|
Adults at enrolment (age ≥ 18). French as a native language. HD diagnosed and confirmed by genetic test. Manifest HD at stage 1-2 (UHDRS ≥ 5 and 6 < TFC ≤ 13). Provided written informed consent or consent from a legally authorized representative. Contraception for women of childbearing age. | Involvement in an interventional research study modifying the management approach. Pre-existing conditions that may disrupt cognition (stroke, traumatic brain injury, active epilepsy, learning disorders, alcohol dependence syndrome, substance abuse, psychiatric disorders), severe cognitive impairment (MMSE <16), clinically significant pathological state which could compromise the subject’s safety or the assessment of study outcomes. Pregnant or lactating women. Individuals deprived of liberty by administrative or judicial decision. Individuals undergoing psychiatric care under constraint. Individuals not affiliated with or not beneficiaries of a social security system. |
Legend: Huntington’s disease (HD) ; Unified Huntington’s disease rating scale – total motor score (UHDRS) ; Total functioning capacity scale (TFC) ; Mini mental state examination (MMSE)
Considering the study’s context within a population prone to cognitive impairments, provisions are made to include patients who may be under legal guardianship or who may not be capable of providing consent. Therefore, for patients unable to consent, the inclusion process (provision of information and consent collection) can be conducted with the assistance of a legally authorized representative. The date of information, the reflection period, and the date of consent signature by both parts are documented in the patient’s source file. The present study was approved by Ethical Committee South-East IV of Léon Bérard Centre n°25.00332.000366 on 25/04/2025 and was recorded as a Clinical Trial (NCT06807892) on 29/01/2025. It will be conducted in accordance with the Declaration of Helsinki.
Randomization procedure
The allocation of care (SYN or SEQ) is conducted through simple randomization (allocation ratio of 1:1) balanced by blocks of random sizes (from 2 to 10). The randomization procedure is performed by the Biostatistics and Methodology Unit of the CHU. Patients are randomized after the first evaluation phase (V0) using the randomization module in Ennov Clinical®. The patients included in the study are randomly assigned to one of the two training groups. The result of the randomization procedure is concealed to every participant but during training sessions they can guess their group allocation with the type of exercise experienced.
Sample size and withdrawal
As this work is an exploratory study, we based our sample size calculation on effect sizes (ES) found in comparable studies that investigated effectiveness of motor-cognitive training. The systematic review from Huynh et al., has two studies with small-moderate ES on global cognition. However, these studies are based on a 9-month motor-cognitive training with pre-manifest HD patients (Huynh et al., 2022). The meta-analysis of Embrechts et al., concerns stroke patients but it gives an overall small ES (g=0.22) on motor and cognitive functions in favour of SYN training (Embrechts et al., 2023). Supposing that we planned a future two-armed parallel group randomized clinical trial with a two-sided Type I error rate of 5% and, a power of 80% and a small ES (0.1 ≤ ES ≤ 0.3), we need 20 participants per group for a pilot randomized trial (Whitehead et al., 2016). Considering a maximal dropout rate of 10%, a minimum of 45 participants will be recruited at the CNRMN. Given constraints related to equipment loans and availability of eligible participant, a recruitment duration of 2 years is anticipated. Patients may withdraw from the study at any time.
Interventions
Treatment delivery
In both groups, the first session is conducted at the patient’s home with one of the two study supervisors (either a psychologist specialized in neuropsychology or a professional in adapted physical activity who is involved in the coordination of the present study). The purpose of this initial supervised session is to introduce the patient to the equipment, the program, the exercises, and the exergame that will guide him throughout the training process. Additionally, the goal of this first supervised session is to ensure the initial exercise parameters (display and response times, etc.) are appropriately tailored to the patient’s level, to verify understanding of the instructions, to ensure correct execution of movements, and to reinforce adherence to safety instructions. Subsequent sessions are conducted independently by the patient at their home. A brochure containing safety guidelines and contact information for the supervisors in case of questions is provided to participants at the beginning of the study. Moreover, a monthly phone call is scheduled to ensure participant’s involvement in the training program and to discuss about potential technical problems.
Design of exercises and sessions
Each SEQ exercise targets a specific motor function (balance, muscle strengthening, walking) or cognitive function (flexibility, inhibition, working memory). Six exercises per cognitive function and nine per motor function have been created. For the SYN group, each cognitive exercise was combined with three motor exercises leading to fifty-four possibilities (see Table A.1 in supplementary material for SEQ and SYN exercises descriptions). Motor and cognitive exercises have different levels of difficulty that evolve independently. Each motor exercise is associated with a specific type of difficulty, including 3 levels. Types of difficulty are the amplitude of the movement, the speed of execution or the maintenance/repetition of the movement. For cognitive exercises, difficulty progresses following a specific number of successively good responses during the exercise. For inhibition and flexibility exercises, after 2 good answers in a row, the difficulty is incremented (e.g. decreasing response time or stimuli display). For the working memory exercises, the participant must correctly solve 3 exercise’s cycles during a session to increase the level of difficulty for the next session (e.g. after 3 correct recalls in a backward span task, the number of stimuli will increase during the next session).
The sessions are offered individually at home, with each session lasting approximately 60 minutes, three times per week for 12 weeks. These sessions consist of 10 minutes of motor warm-up (i.e. articular rotations) at the beginning, 40 minutes of motor and cognitive exercises (SYN or SEQ), and 10 minutes of muscle stretching and relaxation at the end. In the SYN intervention, the 40 minutes of exercises involve simultaneous motor and cognitive stimulation. In the SEQ intervention, exercises are performed sequentially: 20 minutes of motor exercises and 20 minutes of cognitive exercises. Regardless of the training group, each session stimulates both motor and cognitive functions. Their presentation order is randomized (see Table 2).
Table 2 - Example of a weekly planning for both trainings
SYNERGICAL TRAINING | SEQUENTIAL TRAINING | ||
|---|---|---|---|
Session 1 | Flexibility + Walking Inhibition + Balance Working Memory + Strength | Session 1 | Flexibility Walking Inhibition Balance Working Memory Strength |
Session 2 | Inhibition + Strength Working Memory + Walking Flexibility + Balance | Session 2 | Inhibition Strength Working Memory Walking Flexibility Balance |
Session 3 | Working Memory + Balance Flexibility + Strength Inhibition + Walking | Session 3 | Working Memory Balance Flexibility Strength Inhibition Walking |
Description of the exergame
The exergame, named “CogniMove” was developed in the Plateforme Angevine d’Analyse des Comportements (P2AC - University of Angers, France) using the game engine Unity (Unity Technologies). The system is composed of a laptop (Latitude 3510, Dell Technologies Inc.), a Bluetooth gamepad (Slim wireless keypad, Satechi®) and a 3-dimensional camera (Astra Pro Plus, Orbbec Inc.) (see Figure 2). The gamepad allows to navigate into the exergame and is necessary for solving cognitive exercises, particularly in the SEQ group. The camera identifies the participant’s body and displays it as a skeleton on bottom right corner of the screen. Thus, the participant can adjust his position to perform motor exercises optimally. The camera detects also correct movement patterns according to the exercise. Algorithms were elaborated to recognize a specific movement by comparing positions of different joints. For example, for the squat exercise, the exergame will identify a correct execution when the distance between hips and ankles decreases. As the distance is shortened, the amplitude of the squat increases as well as the level of motor difficulty. Therefore, specific algorithms were created to identify each motor exercise, including the different levels of difficulty.

Figure 2 - CogniMove system (A – Laptop ; B – Gamepad ; C – Camera) and main interface (D)
We implemented exergame features that can support training adherence, thus exercise benefits (Manser et al., 2025). The presence feedbacks allows participants to be informed about their performance and progression throughtout exercises. In CogniMove, HD patients have a instaneous feedback of their motor execution (i.e. difficulty level of the movement) and a percentage of correct answer, for the cognitive exercise, at the end. This functionality helps to motivate the participant to reach better performances. In addition, we constructed CogniMove around the japanese universe. The game interface contains different avatars and landscapes relating to the medieval period and different fun facts of the japanese culture and history appear at the end of an exercise or when navigating through the exergame. These features enrich the environment and participate to the gamification of the training program (Matallaoui et al., 2017).
Exercises content
Our training program, regardless of the group (SEQ or SYN), is designed to address specific motor and cognitive functions affected by HD. Balance, strength, and gait will be targeted for motor aspects (Cruickshank et al., 2014) and EF (inhibition, flexibility, working memory) for cognitive aspects which are the earliest cognitive impairment in HD (Verny et al., 2007).
SYN exercises combine physical activity and cognitive stimulation simultaneously. The objective of these exercises is to perform or solve a cognitive task through a specific motor task (e.g., Go/No-go with squats as the Go stimulus and waiting position as the No-go).
For instance, to enhance working memory and muscle strength, the patient is requested to count the respective number of two stimuli presented one by one on the screen at random. The patient is required to count the number of stimulus 1 and stimulus 2. To provide response, they must perform x jabs for stimulus 1 and x squats for stimulus 2 (see Figure 3).
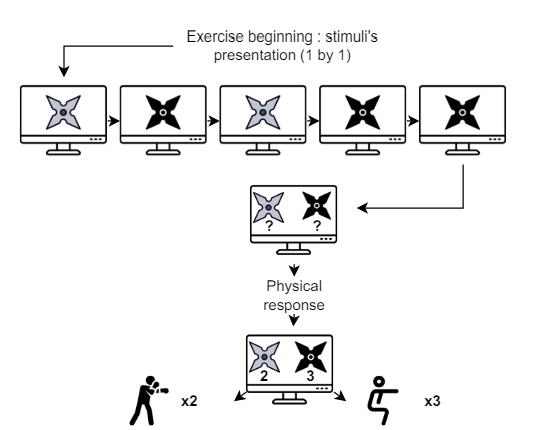
Figure 3 - Example of a synergical exercise
For the SEQ group, motor and cognitive exercises are displayed one after the other. The patient first engages in 20 minutes of motor training (muscle strengthening, balance, and walking) followed by 20 minutes of cognitive training (inhibition, working memory, and flexibility). The exercises are performed independently of each other.
For example, in the first part focusing on cognitive exercises, to work on working memory, the patient is asked to count the number of two stimuli presented on the screen randomly. To give the response, the patient has to click on a numeric pad: press button A twice to indicate that stimulus 1 appeared twice and press the button B three times to indicate that stimulus 2 appeared three times.
Following the completion of the cognitive exercise, the motor exercise begins. For instance, to enhance muscle strength, the patient has to perform jabs and squats in accordance with the number indicated on the screen (see Figure 4).
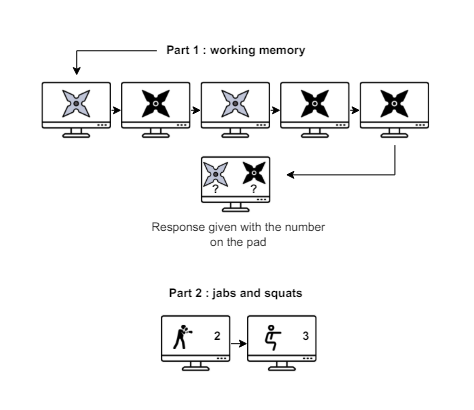
Figure 4 - Example of sequential exercises
Assessment
To study the temporal evolution of the various outcome measures, an assessment lasting approximately 2.5 hours is conducted for all participants at the following time points: the inclusion visit (V0), the post-intervention visit conducted within 2 weeks after the last session (V1), and the last visit that is planned 3 months after the end of the program (V2). This assessment is conducted by a neuropsychologist and a professional in adapted physical activity within the CNRMN.
Feasibility and acceptability
The acceptability and feasibility of both programs are evaluated based on the number of completed sessions, dropout rate, quality of responses, level achieved in each exercise, session completion (yes/no), early session termination, session duration, and through open-ended questions. These questions inquire about the attractiveness of the program (motivation), clarity, effectiveness, reliability of exercises (safety), and hedonic quality (creativity, stimulation) of the program. Patients must answer these questions on a scale ranging from 0 (strongly disagree) to 5 (strongly agree) (see Table A.2 in supplementary material for more details). Additionally, participant’s satisfaction with the program is rated on a Lickert scale: “How would you rate the program and its support overall?” on a scale from -5 (poor) to 5 (good). An open-ended question allows participants to provide comments to justify the rating given (“Can you justify your rating in a few words?”).
Cognitive function
Cognitive assessments focus on EF and rely on tasks from the Unified Huntington’s Disease Rating Scale (UHDRS) (Kieburtz et al., 1996), including the Stroop test, Symbol Digit Modalities Test (SDMT), Trail Making Test (TMT), and verbal fluency tasks. These tasks emphasize inhibition, flexibility, and processing speed. In the Stroop task, three boards are presented to the subject. The first one involves naming colours (blue, green, or red), the second involves reading words (blue, green, or red), and on the third board, the subject has to inhibit reading the word and instead he/she has to name the ink colour (e.g., “blue” written in red ink). The goal of the SDMT is to correctly associate as many numbers with their corresponding symbols as possible within 90 seconds. During verbal fluency tasks, the subject has first to list as many words from a semantic category as possible in one minute (semantic fluency) and then list as many words as possible beginning with the letters P, R, and V in one minute (phonological fluency). The TMT requires the subject to connect numbers from 1 to 25 as quickly as possible. In Part B, the subject has to alternate between numbers and letters while maintaining ascending numerical order and alphabetical order.
To complete the assessment of EF targeted in our program, working memory is evaluated using the “Digit Span” subtest of the Wechsler Adult Intelligence Scale-Fourth Edition (WAIS IV). This subtest is divided into three sections, with the objective of first one repeating orally dictated numbers in the same order, then in reverse order, and finally in ascending order. The length of the number sequence increases gradually for each step, and the exercise is stopped after two consecutive errors in the same item.
Lastly, overall cognitive function is assessed using the Mini-Mental State Examination (MMSE) (Folstein et al., 1975). Scores range from 0 to 30, with higher scores indicating better cognitive performance.
Motor function
The assessment of physical function focuses on involuntary motor impairments, balance, gait, and strength endurance. For involuntary motor impairments, we will use the Unified Huntington’s Disease Rating Scale-Total Motor Score (UHDRS-TMS), a subscale of the UHDRS designed to clinically monitor the progression of motor impairments specific to HD (Mestre et al., 2018c). Balance will be evaluated using the Berg Balance Scale (BBS), a 14-item scale assessing both static and dynamic balance capacities (Berg, 1989). A better score indicates better balance capacities (maximal score of 56 points). Gait endurance will be assessed through the 6 Minutes Walking Test (6MWT), where participants walk as far as possible in a 30 meter corridor within 6 minutes (Chan & Pin, 2019). These two tests are recommended for evaluating functional capacities in HD (Mestre et al., 2018a). Finally, strength endurance will be evaluated using the 30 Seconds Chair Sit to Stand test (30sec CSTS), which involves standing up and sitting down as many times as possible without assistance for 30 seconds (Jones et al., 1999).
Psychiatric aspects
Anxiety and depression will be assessed using the Hospital Anxiety and Depression Scale (HADS). This self-report questionnaire is commonly utilized and recommended in clinical settings for individuals with Huntington’s disease (HD) (Mestre et al., 2016). The short version of the Problem Behaviours Assessment for Huntington’s Disease (PBA-HD) will be employed to highlight behavioural and psychiatric disturbances. This scale specifically targets symptoms commonly observed in HD, including depression, suicidal ideation, anxiety, irritability, aggressive behaviour, apathy, perseverative thoughts, obsessive-compulsive symptoms, paranoia, hallucinations, and disorientation. The use of this scale is also suggested within the scope of research on HD (Mestre et al., 2016).
Quality of life
The QoL will be assessed using the Short Form Health Survey Questionnaire-12 item (SF-12), which is an abbreviated version of the Medical Outcomes Study Short-Form General Health Survey (Gandek et al., 1998). The SF-12 comprises 12 questions distributed across the same 8 domains (physical and social functioning, limitations due to physical and emotional problems, mental health, vitality, pain, general health perception), with results ranging from 0 (very poor health) to 100 (very good health) on a scale. The use of this questionnaire is recommended for individuals with HD (Mestre et al., 2018b).
Statistical analysis
In line with the extension for pilot trials of the Consolidated Standards of Reporting Trials (CONSORT), feasibility outcomes will be reported descriptively and narratively (Eldridge et al., 2016). Quantitative variables will be described using their mean and standard deviation for normally distributed variables, or their median and interquartile range and minimum/maximum otherwise. The sample size and frequency (with a 95% confidence interval) will be used to describe qualitative variables. Statistical analysis will be performed by the two study supervisors with R software (R foundation for statistical computing, Vienna, Austria). Physical, cognitive, psychiatric outcomes and QoL at V0, V1 and V2 will be analysed using linear mixed models adjusted to variables like age, sex, repetition of cytosine-adenine-guanine triplets, score at the Total Functioning Capacity scale and cognitive status (score at the MMSE). These models will be performed using the lme function from the nlme package (Pinheiro & Bates, 2000). In a first step, models will be performed, for each cognitive, physical, and psychiatric outcomes of interest, without interaction (Time*Group) effect to evaluate the preliminary effectiveness of motor-cognitive training. In a second step, models will be performed with the interaction effect to compare the evolution between the SEQ group and the SYN group, at V1 and V2 (see Figure A.1. in supplementary material for model’s structures in R software). Linearity, normality, and collinearity of data will be graphically checked using the check_model function (Lüdecke et al., 2021). Qualitative variables will be compared using the Chi² Test. For this study, a p<0.05 will be considered as statistically significant.
Discussion
This study aims to evaluate the feasibility and effects of two motor-cognitive training (SYN and SEQ) on physical, cognitive, psychiatric symptoms, and QoL in people with HD and to identify which training is the best to prevent disease’s progression. To the best of our knowledge, this will be the first study to assess, in manifest early stage HD population, the adherence and relevance of two motor-cognitive training programs with specific targets (balance, walking, muscle strength, and EF). It will also be the first trial combining motor and cognitive training through exergaming in HD despite its interest in other population like older adults (Wollesen et al., 2020; Gavelin et al., 2021; Torre & Temprado, 2022) and neurodegenerative diseases (Fritz et al., 2015; Wajda et al., 2017; Johansson et al., 2023).
The exergame and motor-cognitive trainings are anticipated to be well tolerated by patients with few dropout rates, good adherence, and positive feedback. These assumptions are based on previous studies in older adults and adults with Parkinson’s disease that highlighted the feasibility and usability of exergame-based motor-cognitive training (Barry et al., 2014; Manser et al., 2023). In addition, improvements in physical, cognitive, psychiatric symptoms, and QoL are expected in both motor-cognitive training groups. However, higher effects are awaited in the SYN group compared to the SEQ group. Simultaneous training as SYN seems to be more effective than SEQ training on physical and cognitive functions (Gavelin et al., 2021). In fact, the neurophysiological effects (i.e., neuroplasticity, neurogenesis, synaptogenesis) of SEQ training depend on several parameters such as the order and temporal proximity of motor and cognitive exercises. In contrast, in simultaneous training, whether it is SYN or DT, the “facilitation effects” of physical activity and the “guidance effects” of cognitive training are combined within a single exercise. This potentially leads to a superiority of synchronous training over sequential training, but these results require further investigations (Fissler et al., 2013; Herold et al., 2018). From a daily-life perspective, SYN exercises are closer to real-life situations than SEQ ones. For example, walking in a supermarket to buy some food or driving a car are SYN tasks. It demands to solve cognitive tasks by moving. Thereby, SYN exercises can be perceived more meaningful for HD patients, therefore improving adherence and training benefits (Herold et al., 2018).
For the simultaneous form of motor-cognitive, we choose SYN instead of DT because neuroplastic effects (and consequently on cognition and motor skills) are believed to be more beneficial when incorporating a cognitive task into a motor task (SYN) rather than adding a cognitive task to a motor task (DT) (Herold et al., 2018). Furthermore, as mentioned previously, a SYN task is closer to activities of daily living than DT task. For example, HD patients are more able to explore aisles of a supermarket while remembering their list of furniture than solving arithmetic tasks while walking. On the other hand, a SYN exercise does not induce task prioritisation effects like a DT exercise. This effect influences motor or cognitive performance depending on which task is prioritised. Consequently, given the known attentional difficulties in HD (Thompson et al., 2010), the choice of a SYN training seems more appropriate. However, comparative studies on motor and cognitive performances between SYN and DT exercises, particularly on accuracy and reaction time, are essential to clarify this point.
Several studies have demonstrated the relationship between EF and motor abilities such as balance and gait in older adults. Indeed, better executive functioning is correlated with improved balance capabilities and better gait parameters such as speed or variability (Iersel et al., 2008; Ijmker & Lamoth, 2012; Kearney et al., 2013). Moreover, there is a relationship between physical activity and the enhancement of EF in older adults (Chen et al., 2020; Xiong et al., 2021) and patients with Alzheimer’s disease (Zhu et al., 2020). It can be explained by the various neuronal links between motor and cognitive capacities (e.g. frontosubcortical circuits) (Marusic et al., 2018). However, as this existing relationship is currently weak, further trials are needed. Thus, our study, focusing on training capacities such as balance, gait, and EF, will shed light on these relationships among individuals with HD.
Acknowledgements
We want to highlight the contributions of Florian Focone (PhD and manager of the Plateforme Angevine d’Analyse des Comportements) and Axel Barault for the conception and development of the exergame. Preprint version 2 of this article has been peer-reviewed and recommended by Peer Community In Health & Movement Sciences (https://doi.org/10.24072/pci.healthmovsci.100201; Giannouli, 2025).
Ethics approval and consent to participate
The present study was approved by Ethical Committee South-East IV of Léon Bérard Centre n°25.00332.000366 on 25/04/2025 and was recorded as a Clinical Trial (NCT06807892) on 29/01/2025. It will be conducted in accordance with the Declaration of Helsinki. All volunteers will receive an information letter, will have the possibility to discuss any questions they have with medical personnel and, if willing to participate, will sign an informed consent before being enrolled in the study.
Funding
To conduct this study, Julien Godard is supported by a PhD scholarship provided by the University of Angers and Le Mans University while Coline Chartier is supported by a PhD scholarship provided by the University Hospital Centre of Angers and Angers-Loire Métropole.
Conflict of interest disclosure
The authors declare that they comply with the PCI rule of having no financial conflicts of interest in relation to the content of the article. The authors declare the following non-financial conflict of interest: Coline Chartier and Professor Philippe Allain are partly employees of the University Hospital Centre of Angers where the study will be conducted. Professor Philippe Allain contributed to decisions regarding study design but will not participate in data collection or statistical analysis.
Data, scripts, code, and supplementary information availability
Supplementary information is available online (https://doi.org/10.5281/zenodo.15856499; Godard et al., 2025).