Inadequate and excessive gestational weight gain (GWG) have emerged as growing epidemiological health concerns affecting a substantial proportion of pregnant women in high-income countries (Johnson et al., 2015 J. L. Johnson; S. L. Farr; P. M. Dietz; A. J. Sharma; W. D. Barfield; C. L. Robbins Trends in gestational weight gain: The Pregnancy Risk Assessment Monitoring System, 2000—2009, American journal of obstetrics and gynecology, Volume 212 (2015) no. 6, p. 806 | DOI J. L. Johnson; S. L. Farr; P. M. Dietz; A. J. Sharma; W. D. Barfield; C. L. Robbins Trends in gestational weight gain: The Pregnancy Risk Assessment Monitoring System, 2000—2009, American journal of obstetrics and gynecology, Volume 212 (2015) no. 6, p. 806 | DOI J. L. Johnson; S. L. Farr; P. M. Dietz; A. J. Sharma; W. D. Barfield; C. L. Robbins Trends in gestational weight gain: The Pregnancy Risk Assessment Monitoring System, 2000—2009, American journal of obstetrics and gynecology, Volume 212 (2015) no. 6, p. 806 | DOI; Goldstein et al., 2017 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI, 2018; Martínez-Hortelano et al., 2020 J. A. Martínez-Hortelano; I. Cavero-Redondo; C. Álvarez-Bueno; M. Garrido-Miguel; A. Soriano-Cano; V. Martínez-Vizcaíno Monitoring gestational weight gain and prepregnancy BMI using the 2009 IOM guidelines in the global population: A systematic review and meta-analysis, BMC Pregnancy and Childbirth, Volume 20 (2020) no. 1, p. 649 | DOI J. A. Martínez-Hortelano; I. Cavero-Redondo; C. Álvarez-Bueno; M. Garrido-Miguel; A. Soriano-Cano; V. Martínez-Vizcaíno Monitoring gestational weight gain and prepregnancy BMI using the 2009 IOM guidelines in the global population: A systematic review and meta-analysis, BMC Pregnancy and Childbirth, Volume 20 (2020) no. 1, p. 649 | DOI J. A. Martínez-Hortelano; I. Cavero-Redondo; C. Álvarez-Bueno; M. Garrido-Miguel; A. Soriano-Cano; V. Martínez-Vizcaíno Monitoring gestational weight gain and prepregnancy BMI using the 2009 IOM guidelines in the global population: A systematic review and meta-analysis, BMC Pregnancy and Childbirth, Volume 20 (2020) no. 1, p. 649 | DOI). The prevalence of excessive GWG (47%) is notably higher than inadequate GWG (23%), as estimated among pregnant women across the United States, Europe, and Asia (Goldstein et al., 2018 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. L. Misso; J. A. Boyle; C. L. Harrison; M. H. Black; N. Li; G. Hu; F. Corrado; H. Hegaard; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women, BMC Medicine, Volume 16 (2018) no. 1, p. 153 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. L. Misso; J. A. Boyle; C. L. Harrison; M. H. Black; N. Li; G. Hu; F. Corrado; H. Hegaard; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women, BMC Medicine, Volume 16 (2018) no. 1, p. 153 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. L. Misso; J. A. Boyle; C. L. Harrison; M. H. Black; N. Li; G. Hu; F. Corrado; H. Hegaard; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women, BMC Medicine, Volume 16 (2018) no. 1, p. 153 | DOI). The high prevalence of both extremes raises significant concerns, as they are associated with a wide range of adverse maternal and offspring health outcomes (Viswanathan et al., 2008 M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI; Siega-Riz et al., 2009 A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI; Mamun et al., 2010 A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI; Li et al., 2013 N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI; Goldstein et al., 2017 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI, 2018; Ren et al., 2018 M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI; Rogozińska et al., 2019 E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI; Ukah et al., 2019 U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI). In women, inadequate GWG is associated with gestational diabetes mellitus and greater risk of mortality (Viswanathan et al., 2008 M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI; Ukah et al., 2019 U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI), while in offspring it is associated with preterm birth, small for gestational age (SGA), and increased risk of perinatal death (Viswanathan et al., 2008 M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI; Siega-Riz et al., 2009 A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI; Li et al., 2013 N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI; Goldstein et al., 2017 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI, 2018; Rogozińska et al., 2019 E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI; Ukah et al., 2019 U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI). Excessive GWG is associated with maternal preeclampsia, caesarian section, gestational diabetes, and mortality (Viswanathan et al., 2008 M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI; Siega-Riz et al., 2009 A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI; Mamun et al., 2010 A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI A. A. Mamun; M. Kinarivala; M. J. O'Callaghan; G. M. Williams; J. M. Najman; L. K. Callaway Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up, The American Journal of Clinical Nutrition, Volume 91 (2010) no. 5, pp. 1336-1341 | DOI; Li et al., 2013 N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI; Goldstein et al., 2017 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI, 2018; Ren et al., 2018 M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI M. Ren; H. Li; W. Cai; X. Niu; W. Ji; Z. Zhang; J. Niu; X. Zhou; Y. Li Excessive gestational weight gain in accordance with the IOM criteria and the risk of hypertensive disorders of pregnancy: A meta-analysis, BMC Pregnancy and Childbirth, Volume 18 (2018) no. 1, pp. 1-9 | DOI; Rogozińska et al., 2019 E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI; Ukah et al., 2019 U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI), as well as large for gestational age (LGA) offspring, macrosomia, and neonatal death (Viswanathan et al., 2008 M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI M. Viswanathan; A. M. Siega-Riz; M. K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr Outcomes of maternal weight gain, Evidence Report/Technology Assessment (2008) no. 168, pp. 1-223 | DOI; Siega-Riz et al., 2009 A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI A. M. Siega-Riz; M. Viswanathan; M.-K. Moos; A. Deierlein; S. Mumford; J. Knaack; P. Thieda; L. J. Lux; K. N. Lohr A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention, American Journal of Obstetrics and Gynecology, Volume 201 (2009) no. 4, p. 339 | DOI; Li et al., 2013 N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI N. Li; E. Liu; J. Guo; L. Pan; B. Li; P. Wang; J. Liu; Y. Wang; G. Liu; A. A. Baccarelli; L. Hou; G. Hu Maternal Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes, PLOS ONE, Volume 8 (2013) no. 12, p. e82310 | DOI; Goldstein et al., 2017 R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI R. F. Goldstein; S. K. Abell; S. Ranasinha; M. Misso; J. A. Boyle; M. H. Black; N. Li; G. Hu; F. Corrado; L. Rode; Y. J. Kim; M. Haugen; W. O. Song; M. H. Kim; A. Bogaerts; R. Devlieger; J. H. Chung; H. J. Teede Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis, JAMA, Volume 317 (2017) no. 21, pp. 2207-2225 | DOI, 2018; Rogozińska et al., 2019 E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI E. Rogozińska; J. Zamora; N. Marlin; A. P. Betrán; A. Astrup; A. Bogaerts; J. G. Cecatti; J. M. Dodd; F. Facchinetti; N. R. W. Geiker; L. A. H. Haakstad; H. Hauner; D. M. Jensen; T. I. Kinnunen; B. W. J. Mol; J. Owens; S. Phelan; K. M. Renault; K. Å. Salvesen; A. Shub; F. G. Surita; S. N. Stafne; H. Teede; M. N. M. van Poppel; C. A. Vinter; K. S. Khan; S. Thangaratinam Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials, BMC Pregnancy and Childbirth, Volume 19 (2019) no. 1, pp. 1-12 | DOI; Ukah et al., 2019 U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI U. V. Ukah; H. Bayrampour; Y. Sabr; N. Razaz; W.-S. Chan; K. I. Lim; S. Lisonkova Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013, PLoS medicine, Volume 16 (2019) no. 12, p. e1003009 | DOI).
One of the most prominent evidence-based guidelines defining adequate GWG ranges was established in 1990 and revised in 2009 by the Institute of Medicine (IOM) (Institute of Medicine & National Research Council, 2009 Institute of Medicine; National Research Council Weight gain during pregnancy: Reexamining the guidelines, The National Academies Collection: Reports funded by National Institutes of Health, National Academies Press (US), Washington (DC), 2009 | DOI). These guidelines provide weight gain targets based on pre-pregnancy body mass index (BMI): women in the “normal” BMI category are recommended to gain 11.5-16.0 kg throughout their pregnancy, while women in the underweight category should gain more weight (12.7-18.2 kg), and women in the overweight or obese categories should gain less (2.7-6.4 or 5.0-9.1 kg, respectively) (Institute of Medicine & National Research Council, 2009 Institute of Medicine; National Research Council Weight gain during pregnancy: Reexamining the guidelines, The National Academies Collection: Reports funded by National Institutes of Health, National Academies Press (US), Washington (DC), 2009 | DOI). The IOM guidelines have been widely adopted across the world, yet high rates of GWG outside recommended ranges persist, highlighting the need to enhance our understanding of the complexity of the determinants of GWG. In its 2009 guideline update, the IOM identified a lack of evidence on GWG among vulnerable populations, as well as disparities related to racial/ethnic and socioeconomic determinants of GWG (Institute of Medicine & National Research Council, 2009 Institute of Medicine; National Research Council Weight gain during pregnancy: Reexamining the guidelines, The National Academies Collection: Reports funded by National Institutes of Health, National Academies Press (US), Washington (DC), 2009 | DOI).
To date, three reviews have explored some socioeconomic status (SES) and psychosocial factors associated with GWG. Campbell et al. (2016) conducted a narrative review examining the association between SES factors (i.e., childhood SES, income, neighbourhood, and rural vs. urban areas) and GWG. The review provided a high-level overview of studies published in English since 2000, citing one study per SES factor associated with GWG. The authors concluded that income, neighbourhood, and rural vs. urban areas influence GWG. Through a systematic review, O’Brien et al. (2018) examined observational studies focusing on the associations between SES factors (i.e., educational attainment, employment, income, social class, poverty, food security, and health insurance status) and GWG. The review included 16 studies published in English between 2009 and 2016. The authors concluded that low educational attainment was generally associated with GWG outside the recommended range, although the results were mixed, with slightly more studies reporting significant associations (8/16) than no significant associations (6/16). Finally, Athar et al. (2021) conducted a scoping review of observational and experimental studies examining the association between various psychosocial factors (including intimate partner violence, lack of social support, financial distress, food insecurity, chronic stress and depression, eating disorders, and low self-esteem) and GWG. They analyzed nine articles published in English between 2015 and 2020 and concluded that all the above-mentioned factors were associated with GWG. These narrative (Campbell), systematic (O’Brien), and scoping (Athar) reviews were limited in scope, covering only four to sixteen articles each and focusing on publications from 2000 to 2020 and did not differentiate between the different contexts of low-, middle-, and high-income countries. There was also considerable variation in the definitions and selection of SES factors and psychosocial concepts, as well as in the design of included studies (observational and/or clinical studies or not specified), the GWG guidelines used, and the reviews’ conclusions. Furthermore, two of the three reviews had significant flaws in their search strategies, such as poorly defined keywords, imprecise study selection methods, and a lack of clear inclusion/exclusion criteria.
To overcome these limitations and to address gaps highlighted in the 2009 IOM review, we conducted a comprehensive scoping review of 157 articles on the structural determinants of GWG among vulnerable populations in high-income countries. We drew on Bourgois et al.’s (2017) ‘structural vulnerability’ framework, which defines structural vulnerability as “an individual's or a population groups' condition of being at risk for negative health outcomes through their interface with socioeconomic, political and cultural/normative hierarchies” (Bourgois et al., 2017 P. Bourgois; S. M. Holmes; K. Sue; J. Quesada Structural vulnerability: Operationalizing the concept to address health disparities in clinical care, Academic Medicine: Journal of the Association of American Medical Colleges, Volume 92 (2017) no. 3, pp. 299-307 | DOI P. Bourgois; S. M. Holmes; K. Sue; J. Quesada Structural vulnerability: Operationalizing the concept to address health disparities in clinical care, Academic Medicine: Journal of the Association of American Medical Colleges, Volume 92 (2017) no. 3, pp. 299-307 | DOI P. Bourgois; S. M. Holmes; K. Sue; J. Quesada Structural vulnerability: Operationalizing the concept to address health disparities in clinical care, Academic Medicine: Journal of the Association of American Medical Colleges, Volume 92 (2017) no. 3, pp. 299-307 | DOI, p. 17). Our review aimed to identify key structural vulnerability factors (SVFs) associated with GWG and explore the extent (volume of literature, countries and years of publication), range (variety of factors covered), and nature (study design and characteristics of assessed populations) of this body of research.
This scoping review drew on an adaptation of Arksey and O’Malley’s framework (Levac et al., 2010 D. Levac; H. Colquhoun; K. K. O'Brien Scoping studies: Advancing the methodology, Implementation Science, Volume 5 (2010) no. 1, p. 69 | DOI D. Levac; H. Colquhoun; K. K. O'Brien Scoping studies: Advancing the methodology, Implementation Science, Volume 5 (2010) no. 1, p. 69 | DOI D. Levac; H. Colquhoun; K. K. O'Brien Scoping studies: Advancing the methodology, Implementation Science, Volume 5 (2010) no. 1, p. 69 | DOI; Daudt et al., 2013 H. M. Daudt; C. van Mossel; S. J. Scott Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework, BMC Medical Research Methodology, Volume 13 (2013) no. 1, p. 48 | DOI H. M. Daudt; C. van Mossel; S. J. Scott Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework, BMC Medical Research Methodology, Volume 13 (2013) no. 1, p. 48 | DOI H. M. Daudt; C. van Mossel; S. J. Scott Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework, BMC Medical Research Methodology, Volume 13 (2013) no. 1, p. 48 | DOI) and used an iterative process for refining the research question and identifying the SVFs. An information specialist and the lead researchers collaboratively identified an a priori list of factors and keywords associated with the structural vulnerability framework (see Table S1). Psychological and biological factors were not included in our choice of factors. An initial compilation of SVFs was performed among the eligible studies during the selection process, which was then subjected to thorough analysis. This process resulted in the final identification of eight SVFs, namely race/ethnicity, age, parity, marital status, income, education, immigration status and abuse (physical, psychological, and/or sexual). For this review, race and ethnicity are understood as social constructs that are often employed as identifiers in research on health inequalities. These socially constructed categories have “true biological consequences through racism” (Lin et al., 2021 J. S. Lin; L. Hoffman; S. I. Bean; E. A. O’Connor; A. M. Martin; M. O. Iacocca; O. P. Bacon; M. C. Davies Addressing racism in preventive services: Methods report to support the US Preventive Services Task Force, JAMA, Volume 326 (2021) no. 23, pp. 2412-2420 | DOI J. S. Lin; L. Hoffman; S. I. Bean; E. A. O’Connor; A. M. Martin; M. O. Iacocca; O. P. Bacon; M. C. Davies Addressing racism in preventive services: Methods report to support the US Preventive Services Task Force, JAMA, Volume 326 (2021) no. 23, pp. 2412-2420 | DOI J. S. Lin; L. Hoffman; S. I. Bean; E. A. O’Connor; A. M. Martin; M. O. Iacocca; O. P. Bacon; M. C. Davies Addressing racism in preventive services: Methods report to support the US Preventive Services Task Force, JAMA, Volume 326 (2021) no. 23, pp. 2412-2420 | DOI, p. 2417). While both concepts are discussed together due to their overlapping meanings, we acknowledge their distinct significance in specific research contexts: ethnicity is often linked to a person’s cultural identity, whereas race generally refers to broad categories of people divided based on ancestral origins and physical characteristics (Flanagin et al., 2021 A. Flanagin; T. Frey; S. L. Christiansen; AMA Manual of Style Committee Updated guidance on the reporting of race and ethnicity in medical and science journals, JAMA, Volume 326 (2021) no. 7, pp. 621-627 | DOI A. Flanagin; T. Frey; S. L. Christiansen; AMA Manual of Style Committee Updated guidance on the reporting of race and ethnicity in medical and science journals, JAMA, Volume 326 (2021) no. 7, pp. 621-627 | DOI A. Flanagin; T. Frey; S. L. Christiansen; AMA Manual of Style Committee Updated guidance on the reporting of race and ethnicity in medical and science journals, JAMA, Volume 326 (2021) no. 7, pp. 621-627 | DOI). Additionally, age is understood as an SVF, rather than merely a biological factor, as age-related stigma—particularly for pregnant adolescents—along with social policies that overlook age, can increase health risks associated with pregnancy (SmithBattle, 2020 L. SmithBattle Walking on eggshells: An update on the stigmatizing of teen mothers, MCN. The American journal of maternal child nursing, Volume 45 (2020) no. 6, pp. 322-327 | DOI L. SmithBattle Walking on eggshells: An update on the stigmatizing of teen mothers, MCN. The American journal of maternal child nursing, Volume 45 (2020) no. 6, pp. 322-327 | DOI L. SmithBattle Walking on eggshells: An update on the stigmatizing of teen mothers, MCN. The American journal of maternal child nursing, Volume 45 (2020) no. 6, pp. 322-327 | DOI).
Other SVFs, beyond the eight retained in our review, were also identified as being associated with GWG; these included employment and working conditions, adverse childhood events, food security, social support, neighbourhood composition and characteristics, familial responsibilities, language preference, and opportunities for upward mobility. However, these SVFs were reported at a low frequency in the literature (one to six studies in total per factor) and were operationalized such that the findings were difficult to compare between studies. Therefore, these SVFs were not included in our analyses. Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) guidelines were used to ensure comprehensive reporting (Tricco et al., 2018 A. C. Tricco; E. Lillie; W. Zarin; K. K. O'Brien; H. Colquhoun; D. Levac; D. Moher; M. D. J. Peters; T. Horsley; L. Weeks; S. Hempel; E. A. Akl; C. Chang; J. McGowan; L. Stewart; L. Hartling; A. Aldcroft; M. G. Wilson; C. Garritty; S. Lewin; C. M. Godfrey; M. T. Macdonald; E. V. Langlois; K. Soares-Weiser; J. Moriarty; T. Clifford; Ö. Tunçalp; S. E. Straus PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation, Annals of Internal Medicine, Volume 169 (2018) no. 7, pp. 467-473 | DOI A. C. Tricco; E. Lillie; W. Zarin; K. K. O'Brien; H. Colquhoun; D. Levac; D. Moher; M. D. J. Peters; T. Horsley; L. Weeks; S. Hempel; E. A. Akl; C. Chang; J. McGowan; L. Stewart; L. Hartling; A. Aldcroft; M. G. Wilson; C. Garritty; S. Lewin; C. M. Godfrey; M. T. Macdonald; E. V. Langlois; K. Soares-Weiser; J. Moriarty; T. Clifford; Ö. Tunçalp; S. E. Straus PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation, Annals of Internal Medicine, Volume 169 (2018) no. 7, pp. 467-473 | DOI A. C. Tricco; E. Lillie; W. Zarin; K. K. O'Brien; H. Colquhoun; D. Levac; D. Moher; M. D. J. Peters; T. Horsley; L. Weeks; S. Hempel; E. A. Akl; C. Chang; J. McGowan; L. Stewart; L. Hartling; A. Aldcroft; M. G. Wilson; C. Garritty; S. Lewin; C. M. Godfrey; M. T. Macdonald; E. V. Langlois; K. Soares-Weiser; J. Moriarty; T. Clifford; Ö. Tunçalp; S. E. Straus PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation, Annals of Internal Medicine, Volume 169 (2018) no. 7, pp. 467-473 | DOI).
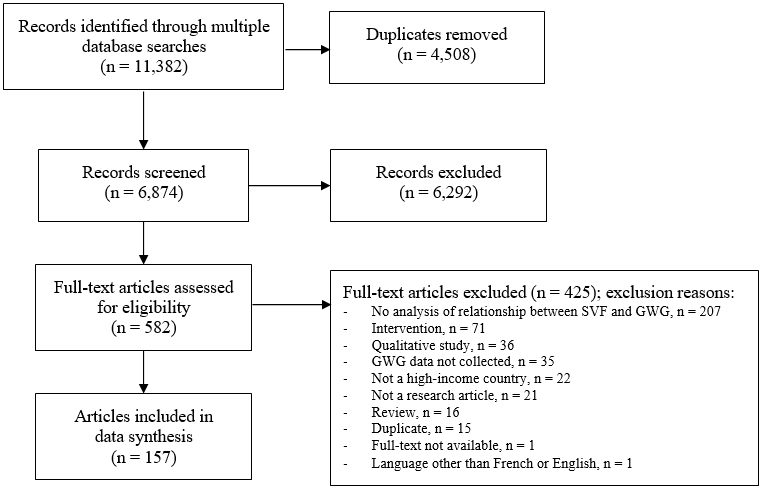
The articles included in this review needed to focus on pregnant women, with at least a subsample of women in each study having experienced one or more SVF. Studies were limited to those with an observational design (prospective, retrospective, or cross-sectional) that used inferential statistics to analyze the relationship between SVFs and GWG. Descriptive studies without statistical comparison were not included in this review. Only peer-reviewed articles published in high-income countries, as classified by The World Bank The World Bank World Bank Country and Lending Groups – World Bank Data Help Desk (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups) | DOIin 2018 (The World Bank), were considered. We limited our analysis to studies conducted in high-income countries to minimize variability arising from different social, cultural, and political contexts. Studies published in languages other than English or French, as well as conference abstracts, were excluded (see Figure 1 for reasons of exclusion).
Electronic searches were performed by an information specialist (coauthor KF) from inception of databases up to October 22nd, 2018, and updated August 1st, 2019 in MEDLINE(R) ALL (1946 to July 30th 2019, Ovid), EMBASE (1947 to July 30th, 2019, Ovid), PsycINFO (1806 to July Week 4 2019, Ovid), CINAHL (1976 to 2019, EBSCOhost), and Sociological Abstracts (1904 to 2019, Proquest). Studies were identified using a combination of each database’s unique subject headings and keywords pertaining to SVFs and weight gain among vulnerable pregnant women. Databases’ limits were used to remove non-peer-reviewed research when feasible (editorials, comments, letter to the editors) and a limit to English and French languages was applied when possible (see Table S2 for the search strategies). Exact duplicate records (n=4,508) were removed using the automatic feature in EndNote X9 (Thompson Reuters, San Francisco, CA, USA) and close duplicate records (n=15) were reviewed and removed manually.
The impact of the COVID-19 pandemic on SVFs, healthcare and community services, as well as health outcomes is widely documented (Dongarwar et al., 2020 D. Dongarwar; V. B. Ajewole; E. Oduguwa; A. Ngujede; K. Harris; T. U. Ofili; O. A. Olaleye; H. M. Salihu Role of social determinants of health in widening maternal and child health disparities in the era of Covid-19 pandemic, International journal of MCH and AIDS, Volume 9 (2020) no. 3, pp. 316-319 | DOI D. Dongarwar; V. B. Ajewole; E. Oduguwa; A. Ngujede; K. Harris; T. U. Ofili; O. A. Olaleye; H. M. Salihu Role of social determinants of health in widening maternal and child health disparities in the era of Covid-19 pandemic, International journal of MCH and AIDS, Volume 9 (2020) no. 3, pp. 316-319 | DOI D. Dongarwar; V. B. Ajewole; E. Oduguwa; A. Ngujede; K. Harris; T. U. Ofili; O. A. Olaleye; H. M. Salihu Role of social determinants of health in widening maternal and child health disparities in the era of Covid-19 pandemic, International journal of MCH and AIDS, Volume 9 (2020) no. 3, pp. 316-319 | DOI; Goyal et al., 2020 M. Goyal; P. Singh; N. Melana Review of care and management of pregnant women during COVID-19 pandemic, Taiwanese Journal of Obstetrics and Gynecology, Volume 59 (2020) no. 6, pp. 791-794 | DOI M. Goyal; P. Singh; N. Melana Review of care and management of pregnant women during COVID-19 pandemic, Taiwanese Journal of Obstetrics and Gynecology, Volume 59 (2020) no. 6, pp. 791-794 | DOI M. Goyal; P. Singh; N. Melana Review of care and management of pregnant women during COVID-19 pandemic, Taiwanese Journal of Obstetrics and Gynecology, Volume 59 (2020) no. 6, pp. 791-794 | DOI; Wastnedge et al., 2021 E. A. N. Wastnedge; R. M. Reynolds; S. R. van Boeckel; S. J. Stock; F. C. Denison; J. A. Maybin; H. O. D. Critchley Pregnancy and COVID-19, Physiological Reviews, Volume 101 (2021) no. 1, pp. 303-318 | DOI E. A. N. Wastnedge; R. M. Reynolds; S. R. van Boeckel; S. J. Stock; F. C. Denison; J. A. Maybin; H. O. D. Critchley Pregnancy and COVID-19, Physiological Reviews, Volume 101 (2021) no. 1, pp. 303-318 | DOI E. A. N. Wastnedge; R. M. Reynolds; S. R. van Boeckel; S. J. Stock; F. C. Denison; J. A. Maybin; H. O. D. Critchley Pregnancy and COVID-19, Physiological Reviews, Volume 101 (2021) no. 1, pp. 303-318 | DOI; Wei et al., 2021 S. Q. Wei; M. Bilodeau-Bertrand; S. Liu; N. Auger The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis, CMAJ, Volume 193 (2021) no. 16, p. E540-E548 | DOI S. Q. Wei; M. Bilodeau-Bertrand; S. Liu; N. Auger The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis, CMAJ, Volume 193 (2021) no. 16, p. E540-E548 | DOI S. Q. Wei; M. Bilodeau-Bertrand; S. Liu; N. Auger The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis, CMAJ, Volume 193 (2021) no. 16, p. E540-E548 | DOI). Including studies published during the pandemic would have required further consideration of context-dependent or timing-specific factors (e.g., confinement), thus further complexifying the analyses of the results. Therefore, the search strategy was not updated to include research from the COVID-19 period.
Covidence Covidence Covidence systematic review software (https://www.covidence.org/) | DOIsystematic review software (Covidence) was utilized for the study selection process. Initially, all citations underwent title and abstract screening, followed by full-text screening of relevant articles, which was conducted independently by two reviewers at both stages of the process. Discrepancies related to the inclusion and exclusion of articles among reviewers were resolved by the lead researcher in consultation with the reviewers. To ensure consistency and coherence in the interpretation of citations and predetermined eligibility criteria, a calibration exercise was conducted with 75 articles prior to the title and abstract screening. Citations deemed irrelevant at the full-text stage were assigned an exclusion reason.
Data charting and synthesis
Data charting was undertaken in two phases. In the first phase, eligible articles were recorded in a pre-piloted Excel data charting file to extract relevant information, including the study characteristics, GWG assessment, SVF, and key findings related to GWG. The second phase was initiated after the selection of the final eight SVFs. In the data charting file, associations between each SVF and GWG were documented as “S” for significant, “NS” for non-significant, or left blank if the SVF was not assessed. When studies reported both significant and non-significant associations for a specific SVF due to variations between subgroups (e.g., non-significant relationship among normal weight participants but significant relationships among overweight and obese participants), the association was reported as “S & NS” in supplementary material and as significant in the “Results” section below. This approach aimed to ensure that the associations between SVFs and GWG among any subset of women were adequately represented in the review. When multiple statistical models with different adjustments were presented, the most adjusted model was kept for data charting. The iterative process and multiple revisions of each article were instrumental in identifying the final eight factors and ensuring data accuracy.
The final supplementary files, which contain the comprehensive data charting, include information on the first author, year of publication, country, study design, information on GWG (measurement and guideline used), sample characteristics and size, key findings, additional notes, and references. The complete file is available in Table S3.
Terminology associated with GWG
The terminology and reference values associated with GWG guidelines varied according to the publishing date and geographical context. In this review, the terms “inadequate” and “excessive” are used to describe GWG below or above GWG guidelines, respectively, while “adequate” is used to designate GWG that falls within guidelines.
Database searches using the identified criteria yielded 11,382 articles. Following duplicate removal, 6,874 articles were screened for titles and abstracts, 582 articles underwent full-text screening, and 157 articles were included in the final dataset (see Figure 1 for details).
This review identified eight SVFs most frequently studied in relation to GWG: race/ethnicity (58% of articles), age (55%), parity (31%), education (28%), income (25%), marital status (18%), immigration (12%) and abuse (physical, psychological, and/or sexual; 8%). While the influence of race/ethnicity and age on GWG have been studied since the 1970s, other factors gained attention a decade or two later (e.g., 1980s for marital status, and 1990s for parity, income, education, immigration status, and abuse). The IOM 2009 guidelines (Institute of Medicine & National Research Council, 2009 Institute of Medicine; National Research Council Weight gain during pregnancy: Reexamining the guidelines, The National Academies Collection: Reports funded by National Institutes of Health, National Academies Press (US), Washington (DC), 2009 | DOI) were the most commonly used, followed by the IOM 1990 guidelines (Institute of Medicine, 1990 Institute of Medicine Nutrition during pregnancy, National Academy Press, Washington, D.C., 1990 | DOI Institute of Medicine Nutrition during pregnancy, National Academy Press, Washington, D.C., 1990 | DOI Institute of Medicine Nutrition during pregnancy, National Academy Press, Washington, D.C., 1990 | DOI). Other guidelines, such as those determined by a country’s health department, were used in a small segment of studies. GWG was reported either as a continuous outcome or categorized and compared between groups of pregnant women (i.e., one group having a higher or lower GWG than the other) or between GWG adequacy groups (i.e., inadequate, adequate, excessive). The study samples ranged greatly in size, with 46 women in the smallest study and nearly eight million women in the largest study. Most studies (60%) had a retrospective design, 32% were prospective, and 9% were cross-sectional. GWG data were retrieved from medical records (39%), birth certificates (20%), participant self-report (20%), or measured by the study team (17%); five studies (3%) used two different methods for collecting GWG data, and two studies (1%) did not clearly state their GWG collection method. The characteristics of each study and their association with the eight SVFs are shown in Table S3. A synthesis of the studies examined is detailed below and presented in Table 1.
Table 1. Summary of the literature exploring key structural vulnerability factors (SVFs) associated with gestational weight gain (GWG).
Structural vulnerability factor
|
Number of studies assessing specific SVF
|
|
|
Number of studies finding a significant association between the SVF and GWG (%)
|
|
|
|
Australia, Belgium, Canada, Czech Republic, Ireland, Netherlands, New Zealand, Norway, Singapore, Spain, Sweden, Switzerland, USA,
|
|
|
|
|
|
Australia, Austria, Belgium, Canada, Ireland, Japan, Korea, Netherlands, New Zealand, Norway, Saudi Arabia, Singapore, Slovenia, Sweden, Switzerland, Taiwan, USA
|
|
|
|
|
|
Australia, Belgium, Canada, Korea, Netherlands, New Zealand, Singapore, Sweden, Switzerland, USA
|
|
|
|
|
|
Belgium, Canada, Sweden, USA
|
|
|
|
|
|
Canada, Korea, Netherlands, Singapore, USA
|
|
|
|
|
|
Belgium, Canada, Croatia, Korea, Netherlands, Norway, Spain, Sweden, USA
|
|
|
|
|
|
Australia, Canada, France, Ireland, New Zealand, USA
|
|
|
Abuse (physical, psychological, and/or sexual)
|
|
|
|
|
Ninety-one out of the 157 included studies (58%) assessed the relationship between race/ethnicity and GWG (Table S4). Seventy-two studies (79%) found a significant association between GWG and race/ethnicity, whereas 19 studies (21%) found no significant association. Studies were published from 1976 to 2019 and were conducted in the USA (75 studies, 82%), Canada (three studies, 3%), Australia, the Netherlands (two studies each, 2%), Belgium, Czech Republic, New Zealand, Norway, Singapore, Spain, Sweden, and Switzerland (one study each, 1%), and one study (1%) was conducted in multiple countries (New Zealand, Australia, and Ireland). The sample sizes ranged from 56 to 7,966,573 women. Twenty-eight studies (31%) included a population that was primarily affected by an SVF (adolescents, women with a low income, unmarried women, and/or women from a racial/ethnic minority group). The most studied racial or ethnic groups were White, Black, and Hispanic, with 31 studies (34%) specifying both a woman’s racial group and their Hispanic/non-Hispanic identity. One of the least represented groups was Indigenous women.
Eighty-seven out of the 157 studies (55%) considered the association between age and GWG (Table S5). Forty-six studies (53%) found a significant association and 41 studies (47%) found no significant association. A comparison of GWG between adolescents and adults was conducted in 36 of these studies, with 25/36 studies (69%) finding a significant association and 11/36 (31%) finding no significant association. Articles were published from 1977 to 2019 and took place in the USA (67 studies, 77%), Taiwan (3 studies, 34%), Canada, Japan, Korea (2 studies each, 2%), Australia, Austria, Belgium, the Netherlands, Norway, Saudi Arabia, Singapore, Slovenia, Sweden, Switzerland (one study each, 1%), and one study involved three countries (New Zealand, Australia, Ireland). Sample sizes ranged from 55 to 3,960,796 women; thirty-five studies (40%) were specific to women with an SVF (adolescents, women with a low income, women of a racial/ethnic minority group, unmarried women, low education, and/or multiparous women). Age was primarily assessed as a categorical variable, with a diverse range of age categories used (e.g., <25 years vs. ≥25 years; and <20 years, 20-29 years, 30-39 years, and ≥40 years). The age ranges defining adolescence varied between studies, with some studies categorizing women up to the age of 16 as adolescents, while others considered those up to the age of 19 as adolescents.
Forty-eight of the 157 studies (31%) examined the relationship between parity and GWG (Table S6). Significant associations between these factors were reported in 38 studies (79%), while 10 studies (21%) reported no association. Publication years ranged from 1990 to 2019. Studies were conducted in the USA (37 studies, 77%), Canada, Sweden (two studies each, 4%), Australia, Belgium, Korea, the Netherlands, New Zealand, Singapore, and Switzerland (one study each, 2%). The smallest sample size was 55 women, whereas the largest was 2,976,805 women. Twenty-two studies (46%) had a population that primarily included women with an SVF (racial/ethnic minority group, adolescents, and/or women with a low income). The terms ‘nulliparous’ and ‘primiparous’ were often used to refer to women whose first delivery was examined in the study. The GWG of nulliparous or primiparous women was generally compared to that of multiparous women. A more in-depth assessment of parity was performed in 15 studies (31%), in which either more categories of parity were included (e.g., zero, one, two, three or more previous births) or parity was assessed as a continuous variable.
Twenty-eight of the 157 studies (18%) assessed the association between marital status and GWG, with 15 studies (54%) finding a significant association and 13 studies (46%) finding no significant association (Table S7). Studies were published between 1985 and 2019 in the USA (25 studies, 89%), Belgium, Canada, and Sweden (one study each, 4%). Sample sizes ranged from 101 to 251,342 women, with half of the studies involving a population affected by one or more SVF (women with a low income, a racial/ethnic minority group, multiparous, and/or adolescents). Categories used to assess marital status varied between studies; the general categories of ‘married’ and ‘unmarried’ were commonly used, but some studies opted for more specific categories such as ‘married/cohabitating with partner’, and ‘single/separated’, or ‘married/partnered’, ‘separated/divorced’, or ‘single/no partner’.
Thirty-nine of the 157 studies (25%) examined the association between income and GWG (Table S8). Twenty studies (51%) found a significant association, whereas 19 (49%) found no significant association. Article publication years ranged from 1995 to 2019. The studies were conducted in the USA (33 studies, 85%), Canada, Korea (two studies each, 5%), the Netherlands, and Singapore (one study each, 3%). The smallest sample size was 75 women and the largest was 515,148 women. Thirteen studies (33%) were restricted to a population that had one or more SVF (adolescents, women from a racial/ethnic minority group, and/or women with a low income). Studies seldom used the same income categories (e.g., $0-500, $501-1,000, and ≥$1,000; <$20,000 vs. ≥$20,000; or <100% of federal poverty line vs. >100% federal poverty line). Nearly half (18/39) of all studies used a proxy measure to assess a woman’s income status (e.g., use of Medicaid, or enrollment in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) in the USA).
Forty-four of the 157 studies (28%) examined the association between GWG and education level (Table S9). Of these, 34 (77%) reported a significant association whereas 10 (23%) reported no significant association. Studies were conducted between 1992 and 2019 in the USA (33 studies, 75%), Sweden (three studies, 7%), Canada (two studies, 5%), Belgium, Croatia, Korea, the Netherlands, Norway, and Spain (one study each, 2%). The sample sizes ranged from 55 to 2,796,805 participants. Fifteen studies (34%) were specific to women with an SVF (racial/ethnic minority group and/or women with a low income). Education was measured as a continuous variable in three studies (7%), with the remaining studies measuring education as a categorical variable. Categories varied between studies, with some studies including only two categories (e.g., less than high school vs. high school or more), and others including up to five categories (e.g., 0-8 years, 9-11 years, 12 years, 13-15 years, or ≥16 years of education).
Nineteen of the 157 studies (12%) assessed the relationship between immigration status and GWG, with all but one finding significant associations between these factors (Table S10). Studies were published from 1997 to 2018 in the USA (14 studies, 74%), Canada (three studies, 16%), France (one study, 5%), and one study (5%) included multiple countries (New Zealand, Australia, and Ireland). The smallest sample size was 46 women and the largest was 250,857. Nine studies (47%) were limited to women with an SVF (racial/ethnic minority group, adolescent, and/or low-income). Approximately half of the studies considered immigration status as a dichotomous variable (i.e., born in their country of residence or foreign-born), and six studies (32%) categorized women according to their length of time in their country of residence (e.g., US-born, lived in the USA ≥10 years, lived in the USA <10 years). In all six studies, the length of time since a woman’s immigration had a significant effect on GWG.
Physical, psychological, and/or sexual abuse
Twelve of the 157 studies (8%) considered the association between experiencing abuse and GWG (Table S11). Nine studies (75%) found a significant association and three (25%) found no significant association. Studies were published from 1996 to 2017 in the USA (10 studies, 83%), Iceland, and Taiwan (one study each, 8%). Sample sizes ranged from 337 to 251,342 women. Half of the studies included a population with one or more SVF (adolescents, low-income, and/or racial/ethnic minority group). Studies primarily assessed the impact of physical abuse on GWG, but sexual and psychological abuse were also examined. The timing of abuse (e.g., during childhood, before pregnancy, or during pregnancy) and perpetrator of abuse (e.g., intimate partner) were considered in some studies.
This scoping review, focusing on the pre-COVID-19 pandemic period, highlights the extent, range, and nature of the literature on SVFs and GWG in high-income countries. We identified eight SVFs that were most commonly explored in 157 observational studies published between 1976 and 2019 across 22 countries. Most studies were conducted in the USA, used a retrospective design, and examined diverse populations in which a subgroup or the entire sample experienced one or more SVFs. Among all SVFs examined, race/ethnicity was the most extensively studied, with research spanning the longest period (1976-2019) and involving the largest sample size (n=7,966,573). Race/ethnicity had the second-highest proportion of studies reporting a significant relationship with GWG (n=72/91, 79%), surpassed only by immigration status (significant association in n=18/19 studies, 95%). This review also demonstrates a substantial heterogeneity in study contexts, methodologies, populations, and findings, posing a challenge for determining clear trends in the associations between SVFs and GWG across studies. The following sections compare our findings with previous reviews and identify key challenges and considerations for future research.
Comparison with previous reviews
Similar to the findings of Campbell et al. (2016) and Athar et al. (2021), who reported a high prevalence of association between their studied vulnerability factors and GWG, we found that the majority of studies reported significant associations between SVFs and GWG. The proportion of articles in our review reporting significant associations ranged from 51% for those assessing the relationship between GWG and income, to 95% for those examining the association with immigration status. This contrasts with O’Brien et al. (2018), who concluded that only low educational attainment was associated with GWG. However, O’Brien et al. also reported mixed results, with eight out of 16 studies showing significant associations and six showing non-significant associations. Our review also further expands the list of vulnerability factors known to influence GWG, adding the concepts of race/ethnicity, age, parity, marital status, and immigration to the factors previously identified by Campbell, Athar, and O’Brien.
Collecting, analyzing, and comparing GWG
Several methodological challenges need to be acknowledged when comparing a wide breadth of studies examining inadequate or excessive GWG. First, there is substantial heterogeneity in the way that GWG was collected: close to 60% of studies extracted information on GWG from medical records or birth certificates, while most of the remaining studies relied on measurements by researchers or self-reported data. Second, guidelines used to categorize GWG adequacy varied between studies: the most commonly used were the IOM 2009 guidelines, followed by the IOM 1990 guidelines. In fewer than 10% of studies, other GWG guidelines were applied such as guidelines determined by a country’s health department. The use of different guidelines may lead to misclassification of adequate GWG between studies. Third, statistical analyses used to assess the relationship between SVFs and GWG differed between studies, where some examined the influence of SVFs at a superficial level comparing frequencies of inadequate GWG among different groups of women (e.g., vulnerable vs. less vulnerable), while others performed more in-depth analyses using multivariable models with covariate adjustment (e.g., odds of excessive GWG for a racial/ethnic minority group compared to White, adjusted for age, income, education, etc.). As such, confounding variables and covariates were not always controlled for or comparable between studies. Furthermore, comparator groups varied with some studies comparing the likelihood of inadequate GWG to two distinct groups (e.g., adults vs. adolescents), while others assessed it within the same group of women (e.g., likelihood of excessive vs. adequate GWG among adolescents). Finally, most studies (60%) used a retrospective design, which comes with certain limitations, including a lack of control over data collection tools and methods, as well as potential biases related to the selection of participants, recall of information, and confounding factors (Talari & Goyal, 2020 K. Talari; M. Goyal Retrospective studies - Utility and caveats, The Journal of the Royal College of Physicians of Edinburgh, Volume 50 (2020) no. 4, pp. 398-402 | DOI). This heterogeneity in data collection methods, guideline application, and analytical approaches limits the ability to draw direct associations between SVFs and inadequate or excessive GWG across different groups of women.
Defining, categorizing, and comparing structural vulnerability factors
Differences in definitions and categorizations of each SVF add complexity when comparing study findings. Inconsistencies arose in the definition of SVF constructs across studies, often treating groups as equivalent without considering their social context (e.g., equating ‘single’ and ‘unmarried’ women in relationship status comparisons). Additionally, many SVFs have been analyzed as continuous or categorical variables, with differing thresholds and reference groups used across studies. For example, the relationship between age and GWG was analyzed using total years of age or categories such as adults and adolescents (with varying cut points for adolescent and adult age groups). Parity was occasionally examined as a continuous variable, yet most studies dichotomized this SVF into nulliparous and multiparous groups. Income measurements included total household income, percentage of federal income, and poverty-to-income-ratio, while education was reported as total years of education in some studies, and categorized by the highest level of educational attainment in others. The choice of categories may not only affect the observed relationship between the SVF and GWG, but also influences the representation of smaller or more marginalized groups of women, particularly in the case of race/ethnicity. For instance, the relationship between Indigeneity and GWG was not prominently reported in the studies included in our review. Indigenous women were often either excluded from studies (e.g., Cavicchia et al., (2014)), or were grouped in with other racial/ethnic groups (e.g., Headen et al., (2018)). These systematic differences in definitions, categorization, and representation not only inevitably compromise the ability to generate clear comparisons between studies and subsequently to determine the association between each SVF and GWG, but most importantly, also contribute to perpetuate systemic inequalities in health.
Intersectionality and vulnerability
The complexity of analyzing intersecting and overlapping social identities, along with diverse contextual, situational, and geographical factors, contributes to the heterogeneity in defining, categorizing, and comparing SVFs associated with GWG. These socially constructed vulnerability factors are experienced concomitantly and cannot be easily disentangled (Ailshire & House, 2011 J. A. Ailshire; J. S. House The unequal burden of weight gain: An intersectional approach to understanding social disparities in BMI trajectories from 1986 to 2001/2002, Social forces; a scientific medium of social study and interpretation, Volume 90 (2011) no. 2, pp. 397-423 | DOI; Bowleg, 2012 L. Bowleg The problem with the phrase women and minorities: Intersectionality—an important theoretical framework for public health, American Journal of Public Health, Volume 102 (2012) no. 7, pp. 1267-1273 | DOI L. Bowleg The problem with the phrase women and minorities: Intersectionality—an important theoretical framework for public health, American Journal of Public Health, Volume 102 (2012) no. 7, pp. 1267-1273 | DOI L. Bowleg The problem with the phrase women and minorities: Intersectionality—an important theoretical framework for public health, American Journal of Public Health, Volume 102 (2012) no. 7, pp. 1267-1273 | DOI). The intersectional paradigm presents methodological challenges, including selecting appropriate statistical methods, in the study of inequality (Guan et al., 2021 A. Guan; M. Thomas; E. Vittinghoff; L. Bowleg; C. Mangurian; P. Wesson An investigation of quantitative methods for assessing intersectionality in health research: A systematic review, SSM - Population Health, Volume 16 (2021), p. 100977 | DOI A. Guan; M. Thomas; E. Vittinghoff; L. Bowleg; C. Mangurian; P. Wesson An investigation of quantitative methods for assessing intersectionality in health research: A systematic review, SSM - Population Health, Volume 16 (2021), p. 100977 | DOI A. Guan; M. Thomas; E. Vittinghoff; L. Bowleg; C. Mangurian; P. Wesson An investigation of quantitative methods for assessing intersectionality in health research: A systematic review, SSM - Population Health, Volume 16 (2021), p. 100977 | DOI).
Quantitative researchers should be sensitized to the importance and complexity of considering multiple interacting dimensions of social identities that may be relevant in their specific domain (Bauer et al., 2021 G. R. Bauer; S. M. Churchill; M. Mahendran; C. Walwyn; D. Lizotte; A. A. Villa-Rueda Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods, SSM - Population Health, Volume 14 (2021), p. 100798 | DOI G. R. Bauer; S. M. Churchill; M. Mahendran; C. Walwyn; D. Lizotte; A. A. Villa-Rueda Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods, SSM - Population Health, Volume 14 (2021), p. 100798 | DOI G. R. Bauer; S. M. Churchill; M. Mahendran; C. Walwyn; D. Lizotte; A. A. Villa-Rueda Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods, SSM - Population Health, Volume 14 (2021), p. 100798 | DOI). For example, Hoang and Wong (2022) conducted a scoping review on intersectionality in maternal health equity. While none of the 11 quantitative studies fully met intersectionality criteria, Vedam et al.’s study stood out by addressing most of them (Vedam et al., 2019 S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI; Hoang & Wong, 2022). They used a cross-sectional community-based participatory approach to investigate the associations between risk factors such as race, socio-demographics, mode and place of birth, and context of care on mistreatment during pregnancy and childbirth in a large sample (n=2,138) of women in the U.S. (Vedam et al., 2019 S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI S. Vedam; K. Stoll; T. K. Taiwo; N. Rubashkin; M. Cheyney; N. Strauss; M. McLemore; M. Cadena; E. Nethery; E. Rushton; L. Schummers; E. Declercq; the GVtM-US Steering Council The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States, Reproductive Health, Volume 16 (2019) no. 1, p. 77 | DOI). Univariate and bivariate logistic regressions were used to quantify the relationships between risk factors and likelihood of mistreatment, with the intersectional analysis conducted by stratifying the associations between race and mistreatment by various categories of other risk factors. The study exposed variations in maternal mistreatment across individual, social, and pregnancy-related factors and their intersectional approach demonstrated that the likelihood of mistreatment increased when certain risk factors were combined (e.g., women of color with low SES, social risk factors, or pregnancy complications). The researchers also analyzed open-ended responses and provided representative quotes to ensure the voices of mothers were included. However, a systematic review by Bauer et al. (2021) criticizes the use of simplistic statistical methods (e.g., regression with interactions or stratification) that are often incorrectly applied or interpreted in intersectional research. Bohren et al.’s 2024 scoping review on maternal health found that no clinical interventions adopted an intersectional approach, relying instead on unidimensional measures of vulnerability factors (Bohren et al., 2024 M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI). These findings reiterate the need for intersectional research with strong research designs and methodologies, adapted statistical analyses, and finer interpretation of results in the field of perinatal health.
The intersectional lens encourages moving beyond oversimplified approaches when analyzing vulnerability factors that shape pregnancy experience and health outcomes (Bohren et al., 2024 M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI). Although this approach can be complex, it could provide a clearer understanding of within-group diversity and the synergies that produce health inequalities (Bohren et al., 2024 M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI M. A. Bohren; A. Iyer; A. J. D. Barros; C. R. Williams; A. Hazfiarini; L. Arroyave; V. Filippi; C. Chamberlain; T. Kabakian-Khasholian; K. Mayra; R. Gill; J. P. Vogel; D. Chou; A. S. George; O. T. Oladapo Towards a better tomorrow: Addressing intersectional gender power relations to eradicate inequities in maternal health, eClinicalMedicine, Volume 67 (2024) no. 102180 | DOI). For example, a pregnant adolescent might simultaneously face low educational attainment, single marital status, and low income. Trying to isolate the most impactful factor on GWG oversimplifies their interconnectedness within a person’s biography and social context. Huynh et al. demonstrated that excessive GWG was more likely to be experienced by educated Hispanic, and less likely among educated White women, but more common among educated women living in a low or medium socioeconomic neighbourhood (Huynh et al., 2014 M. Huynh; L. Borrell; E. Chambers Maternal education and excessive gestational weight gain in New York City, 1999-2001: The effect of race/ethnicity and neighborhood socioeconomic status, Maternal & Child Health Journal, Volume 18 (2014) no. 1, pp. 138-145 | DOI M. Huynh; L. Borrell; E. Chambers Maternal education and excessive gestational weight gain in New York City, 1999-2001: The effect of race/ethnicity and neighborhood socioeconomic status, Maternal & Child Health Journal, Volume 18 (2014) no. 1, pp. 138-145 | DOI M. Huynh; L. Borrell; E. Chambers Maternal education and excessive gestational weight gain in New York City, 1999-2001: The effect of race/ethnicity and neighborhood socioeconomic status, Maternal & Child Health Journal, Volume 18 (2014) no. 1, pp. 138-145 | DOI). By studying the combination of SVFs with an intersectional approach, we can gain insight into health disparities and better predict the combination of factors, contexts, or living circumstances that place women at greater risk of GWG outside the recommended range.
Varying social contexts of vulnerability factors
While all studies in this review took place in high-income countries, the social, economic, cultural, structural, and political contexts nevertheless vary significantly. For instance, comparing women from different regions of the United States is not equivalent to comparing women between the United States and Japan. Factors like a woman’s racial and ethnic identity are influenced by the social environment, impacting the extent of discrimination or racism she may face. Moreover, the health disparities resulting from immigration depend on factors such as the woman's country of origin, age at immigration, and the duration since immigration, but these aspects are often overlooked in GWG research. These differences inevitably constrain the comparison of GWG when assessing studies on a global scale. For the least studied Indigenous groups, a study may consider other factors such as historical, geographical, and sociopolitical factors. Many of these factors are recognized to be the underlying causes of health inequality through the unequal allocation of power and resources (National Academies of Sciences, Engineering, and Medicine et al., 2017), far surpassing the realms of factors such as age, race/ethnicity, income, and parity. Given these circumstances, it becomes evident that comparisons within specific countries and regions may provide a more accurate portrayal of the association between SVFs and GWG, as this approach enables the consideration of the distinct contextual nuances at play.
Strengths and limitations of the scoping review
This scoping review stands out for its comprehensive inclusion of a substantial range of articles featuring varying populations, methodologies, and statistical approaches. An iterative process was used to refine the research question and identify the final eight SVFs related to GWG. SVFs were developed based on Bourgois’ structural vulnerability framework, and the keywords and search strategy were thoroughly developed by a university librarian (KF) in collaboration with our multidisciplinary research team. To maximize the breath of our search strategy, we used more than 50 keywords and their related terms (see Tables S1 and S2). In contrast, Athar et al. (2021) used a single keyword (psychosocial factors), Campbell et al. (2016) used “socioeconomic or SES,” and O’Brien et al. (2018) used 13 keywords to define SES. Furthermore, our inclusion and exclusion criteria were clearly outlined, unlike Campbell et al. (2016), who did not report any criteria. Our study also included a broader range of populations than previous reviews; for instance, O’Brien et al. (2018) excluded adolescent pregnancies and restricted their review to singleton pregnancies, while Athar et al. (2021) excluded women with preexisting psychiatric or physical comorbidities, while our review did not have these exclusion criteria. By focusing on complex relationships between SVFs and GWG, this scoping review identified possible barriers for research aiming to link independent SVF with GWG, as typically done in systematic or meta-analysis reviews.
Nonetheless, we acknowledge certain limitations. Articles from 2020 and beyond were not included in this review due to the pandemic's unique context. However, including more recent research would likely highlight the importance of intersectionality, especially considering the individual, social, and economic impacts of COVID-19. Studies conducted in low- or middle-income countries were also excluded due to the significant variations in the impacts of SVFs on GWG across vastly different contexts. Consequently, our findings are limited to more affluent environments. Finally, our choice to draw on a broad scope of articles limited the ability to determine the direction of the associations between each SVF and GWG, as inconsistencies between articles regarding many aspects, such as their population characteristics, use of subgroups, and categorization of variables, made the data unsuitable for direct comparison.
This scoping review examined the extent, range, and nature of published associations between eight most commonly studied SVFs and GWG in high-income countries before the COVID-19 pandemic. The review highlights the substantial heterogeneity across study contexts, methodologies, populations, and findings, presenting a challenge for identifying clear trends between SVFs and GWG. In light of this variability, and in line with O’Brien et al. (2018), we suggest that future studies put an emphasis on prospective and objective measures of weight gain during pregnancy. Furthermore, we recommend that subsequent reviews prioritize the synthesis of information from studies conducted with comparable social contexts, populations, and methodologies. Finally, we suggest researchers consider the guiding principles of an intersectional approach by studying clusters of SVFs to better understand how individual characteristics, living conditions, and social contexts collectively influence GWG. Such an approach may help develop a more detailed understanding of the relationship between SVFs and GWG and facilitate the identification of subgroups of women who are at higher risk of inadequate or excessive GWG. This information can be used by healthcare professionals, service providers, and policymakers to help optimize GWG and promote maternal and child health.
The Preprint version 4 of this article has been peer-reviewed and recommended by Peer Community In Health and Movement Sciences of the PCI (https://doi.org/10.24072/pci.healthmovsci.100116; Bernard, 2024 P. Bernard Structural vulnerability factors and gestational weight gain in high-income countries, Peer Community in Health and Movement Sciences, Volume 1 (2024), p. 100116 | DOI P. Bernard Structural vulnerability factors and gestational weight gain in high-income countries, Peer Community in Health and Movement Sciences, Volume 1 (2024), p. 100116 | DOI P. Bernard Structural vulnerability factors and gestational weight gain in high-income countries, Peer Community in Health and Movement Sciences, Volume 1 (2024), p. 100116 | DOI).
Conflict of interest disclosure
The authors declare that they comply with the PCI rule of having no financial conflicts of interest in relation to the content of the article. Bénédicte Fontaine-Bisson is a recommender for PCI Nutrition.
The authors declare that they have received no specific funding for this study.
Data, script, code, and supplementary information availability
Supplementary information is available on Zenodo (https://doi.org/10.5281/zenodo.13311639; Labonté et al., 2024 J. Labonté; A. Dumas; E. Clark; C. Savard; K. Fournier; S. O'Connor; A.-S. Morisset; B. Fontaine-Bisson Supplementary Table for the article: "Structural Vulnerability Factors and Gestational Weight Gain: A Scoping Review on the Extent, Range, and Nature of the Literature" (2024) | DOI J. Labonté; A. Dumas; E. Clark; C. Savard; K. Fournier; S. O'Connor; A.-S. Morisset; B. Fontaine-Bisson Supplementary Table for the article: "Structural Vulnerability Factors and Gestational Weight Gain: A Scoping Review on the Extent, Range, and Nature of the Literature" (2024) | DOI J. Labonté; A. Dumas; E. Clark; C. Savard; K. Fournier; S. O'Connor; A.-S. Morisset; B. Fontaine-Bisson Supplementary Table for the article: "Structural Vulnerability Factors and Gestational Weight Gain: A Scoping Review on the Extent, Range, and Nature of the Literature" (2024) | DOI). No novel data was generated for this study. All data collected from prior studies is collated as Supplementary Tables (see below). No custom scripts or code were used. All Supplementary Tables are indicated in the text with the prefix “S” (e.g., Table S1 for Supplementary Table 1).
-
Table S1: Structural vulnerability factors used for database searches and study screening for a scoping review on the association between structural vulnerability factors and gestational weight gain.
-
Table S2: Search strategy used for each database to identify articles that assessed the relationship between structural vulnerability factors and gestational weight gain.
-
Table S3: Data charting for all studies included in the scoping review.
-
Table S4: Data charting for all studies assessing the association between race/ethnicity and GWG.
-
Table S5: Data charting for all studies assessing the association between age and GWG.
-
Table S6: Data charting for all studies assessing the association between parity and GWG.
-
Table S7: Data charting for all studies assessing the association between marital status and GWG.
-
Table S8: Data charting for all studies assessing the association between income and GWG.
-
Table S9: Data charting for all studies assessing the association between education and GWG.
-
Table S10: Data charting for all studies assessing the association between immigration and GWG.
-
Table S11: Data charting for all studies assessing the association between abuse and GWG.

 CC-BY 4.0
CC-BY 4.0