
 CC-BY 4.0
CC-BY 4.0
Introduction
Neuromuscular electrical stimulation (NMES) training consists of periodically repeated bouts of electrically stimulated muscle contractions and can be used as an alternative or addition to traditional voluntary exercise training regimens in populations where exercise is either not prioritized or feasible (Langeard et al., 2017; Bouguetoch et al., 2021). NMES is usually associated with some level of discomfort, and previous studies have thus used different approaches to muscle activation, with the aim of eliciting strong contractions with minimal discomfort (Rabello et al., 2021; Espeit et al., 2023). Our team has recently investigated the effects of different stimulation parameters (frequency and intensity) and contraction modes (isometric, concentric and eccentric) on experienced pain and ability to elicit torque (Gravholt et al., 2023). In this previous observational study we found that eccentric contractions elicited by high-frequency stimulation (50-100 Hz) where able to evoke high torques above 70 % of maximal voluntary isometric contractions (MVC), while discomfort of participants were kept at a moderate level. This suggests that NMES with eccentric contractions may be a potent training modality for muscle strength and size improvements.
In practice, stimulations will be either superimposed onto voluntary contractions or through NMES alone (Mukherjee et al., 2023). Several studies have examined the effectiveness of electrical stimulation training interventions, generally reporting improvements in muscle strength, muscle size, and physical function in healthy young and older older adults following 3 to 16 weeks of intervention (Rahmati et al., 2021; Mukherjee et al., 2023).
In tailoring training interventions using voluntary activation of musculature, the mode of contraction appears to be an important parameter. This is especially true since stronger associations have been observed, in voluntary training interventions, between concentric/eccentric contractions (compared to that of isometric contractions) and physical function (e.g. movement transitions, walking and climbing stairs) (Lanza et al., 2003; Schoenfeld, 2010; Pedersen et al., 2019; Sieljacks et al., 2020). Voluntary eccentric exercise training has been proposed as an energetically efficient method to induce high mechanical stresses to the musculature, which are well known to elicit substantial increases in both strength and muscle size (Roig et al., 2009; Isner-Horobeti et al., 2013). Nevertheless, almost all electrical stimulation training regimens reported thus far are based on isometric contractions (Langeard et al., 2017; Vitry et al., 2019; Rahmati et al., 2021; Mukherjee et al., 2023).
To our knowledge, no studies have examined whether electrical stimulation training performed with high-torque eccentric contractions is feasible. Hence, the aim of this study was to investigate the feasibility of a training intervention consisting of electrically evoked eccentric contractions of the quadriceps musculature.
Methods
Experimental Approach to the Problem
It was the aim to assess the feasibility of the intervention by measuring retention, completion, drop-outs, and adverse events. Further, a within person pre-post training comparison was used to evaluate strength and muscle composition to provide information for possible future full scale trials. The manuscript has been written with the CONSORT guidelines in mind, the checklist is available alongside data and analysis (Eldridge et al., 2016; Gravholt et al., 2025).
Participants
Eleven persons (4 women and 7 men) where recruited to perform a 4-week electrical stimulation training intervention at a university laboratory. Four participants dropped out during the familiarization phase of the study (age: 27.9 ± 3.5 years old, height: 174.9 ± 8 cm, weight: 72.3 ± 11.3 kg for completers). The inclusion period lasted three months and participants were identified using social media and adverts at university locations. All participants received written and oral information regarding the project prior to their informed consent. Inclusion criteria where: blood pressure in normal range (120/80 ± 10 mmHg) (Chobanian et al., 2003), no known epilepsy, pregnancy or issues regarding mobility and movement of the lower extremities. Further, persons who had resistance trained regularly in the past six months were excluded. All experimental procedures were approved by Region Midtjylland’s ethics committee (#1-10-72-274-19). Participants received monetary compensation for their involvement in the study (approximately 145 USD).
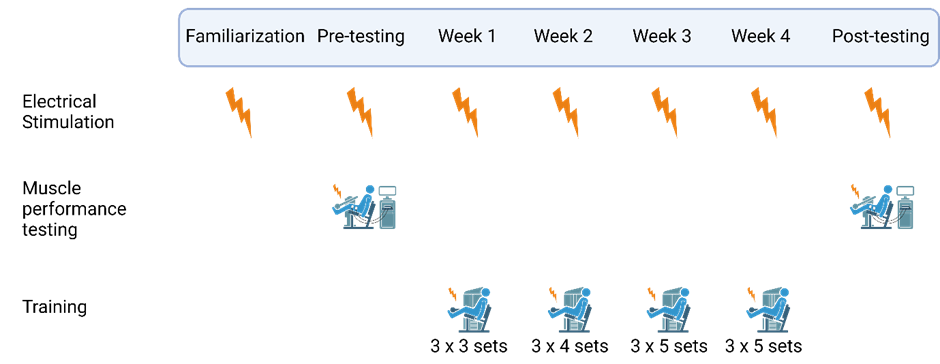
Figure 1 - Schematic of study time line. Each week represents three training sessions. Muscle performance testing includes maximal voluntary contraction, force-velocity testing and the fatigue protocol. Created using Biorender.com under license.
Procedures
One week prior to pre-testing, participants completed two familiarization sessions. The first training session was the first Monday following the pre-test, while the post-test was during the week following the last session. All testing was unilateral using the dominant limb (1 left / 6 right). For an overview, see Figure 1.
Warm-up
Prior to each training and test session, each participant underwent a brief warm-up consisting of 5 minutes of low resistance pedalling on a bike ergometer followed by two times 10 repetitions of full leg extension and -flexion against a low resistance in a dynamometer (Humac NORM, CSMi, Stoughton, MA, USA).
Electrode placement
The placement of electrodes (Biofex CF5090 5 x 9 cm, Biofina A/S, Denmark) was standardized to the participant’s femur length and three visual or palpable landmarks (Botter et al., 2011; Gravholt et al., 2023). Prior to placing the electrodes, the leg was shaved and cleaned with ethanol. The most proximal electrode was placed one third of the length from the posterior superior iliac spine to the superior prominence of the patella, with the middle of the electrode placed between m. rectus femoris and m. vastus lateralis. The two distal electrodes were placed on the muscle belly of m. vastus lateralis and m. vastus medialis, respectively (Maffiuletti et al., 2006). Electrode placement was noted in the participants file and marked on skin following the first day experimental session and used for all future visits. Electrode placement is illustrated in (Gravholt et al., 2023) and the setup in appendix 1.
Maximal Voluntary Isometric Contraction
Participants were seated in the isokinetic dynamometer (Humac NORM, CSI) and settings were noted during the first visit and used for each subsequent training bout or test. Participants were seated at a 90° hip joint angle to the seat and the knee at 70° flexion (0° being full knee extension) during isometric measures. Variable settings include knee adapter length, range of motion for knee flexion and extension. Care was taken to ensure the axis of rotation of the knee was aligned with the axis of rotation of the dynamometer. The protocol for MVIC testing was preceded by a standardized warm-up followed by 3 submaximal attempts where participants were prompted to elicit 50-75% of their MVIC to accustom themselves to the isometric test. Each participant then rested for two minutes prior to the first attempt. Participants were instructed to rest their shin against the padding to ensure an isometric contraction, opposed to the possible brief concentric action in the beginning skewering the rate of force development due to a possible preloading of muscle. Further, they were instructed to contract their muscles as rapidly and explosively as possible until the assessor stopped them after approximately five seconds. The assessor motivated the participant verbally during attempts. Participants rested for two minutes between attempts and were further instructed when needed. A total of three attempts were completed for each participant. The same assessor conducted all tests for a given participant. An average of the two most powerful attempts were used as the measure for MVIC (Sieljacks et al., 2019). Test-retest reliability for MVIC measures was testing in a previous study in our laboratory (Gravholt et al., 2023), and found adequate for both voluntary and electrically stimulated contractions. In one participant, the angle used for the post-test was 10 degrees off, resulting in a greatly decreased MVC, therefore the participant was invited in for a retake of both the pre-fatigued MVC test and the force-velocity-protocol to examine changes in stimulated force output under similar conditions as the pre-test (9 days after the first post). One participant experienced high degrees of muscle soreness after cessation of the training intervention, and was invited for a retake of the post-test protocol as well (7 days after the first post-test).
Maximal Voluntary Dynamic Contraction
In addition to, and following the MVIC testing, participants underwent force-velocity profile testing elicited entirely by electrical stimulations prior to and following a fatiguing protocol of 50 maximal voluntary isokinetic contractions at 60°/s. This was part of an acute intervention seeking to elucidate the fatigue response in high and low frequency electrical stimulations (Herskind et al., 2023). This was completed following MVC testing. The force-velocity testing included 13 contractions at either high or low frequencies (15 and 50 Hz stimulations) and at 0-300°/s. The protocol took 30 minutes to complete. The maximal dynamic force was used as a measure in this study.
Familiarization sessions
Following electrode placement, ultrasound and MVC testing, participants were introduced to electrical stimulation by twitches at 50, 100, 150, 200 and 250 mA with a pulse width of 200 µs using a stimulator box (Model DS7A, Digitimer Electronic, England). Subsequently, using the same progression in intensity, duration of stimulation was increased (up to 1.2 seconds at 50 Hz) and finally the addition of movement was added. Each session lasted approximately one hour.
Electrical stimulation training intervention
Following the initial testing, participants reported thrice a week (usually Monday, Wednesday and Friday in a given week) at Section for Sport Science for their training intervention consisting of electrical stimulation. We strived to maintain one rest-day between sessions, however, if impossible, training was planned on consecutive days. Each training session consisted of unilateral electrically stimulated eccentric contractions in a dynamometer using the same setup as for testing and familiarization. Participants were seated with their knee flexed at 15 degrees, the isokinetic dynamometer was set to begin movement as soon as the contraction commenced and end at 90 degrees of knee flexion, moving at 75 degrees per second. Following warm-up participants received twitches ranging from 50-200 mA to accustom them, followed by 1 second isometric contractions up to their training current to further accustom them. The training protocol for the initial week consisted of 3 sets of 10 eccentric repetitions and was increased to 5 sets of 10 repetitions in the final week of the intervention (see Figure 1). Each eccentric contraction was elicited at 50 Hz, 400 V and 200 µs pulse width for 1.2 second per contraction. No ramping of intensity was used. Stimulation current was determined with the participants to keep discomfort at a tolerable level. Current amplitude was increased throughout the training intervention for all participants. Typical traces are presented from the last session of one participant in
Figure 2. Participants were asked not to co-contract voluntarily.
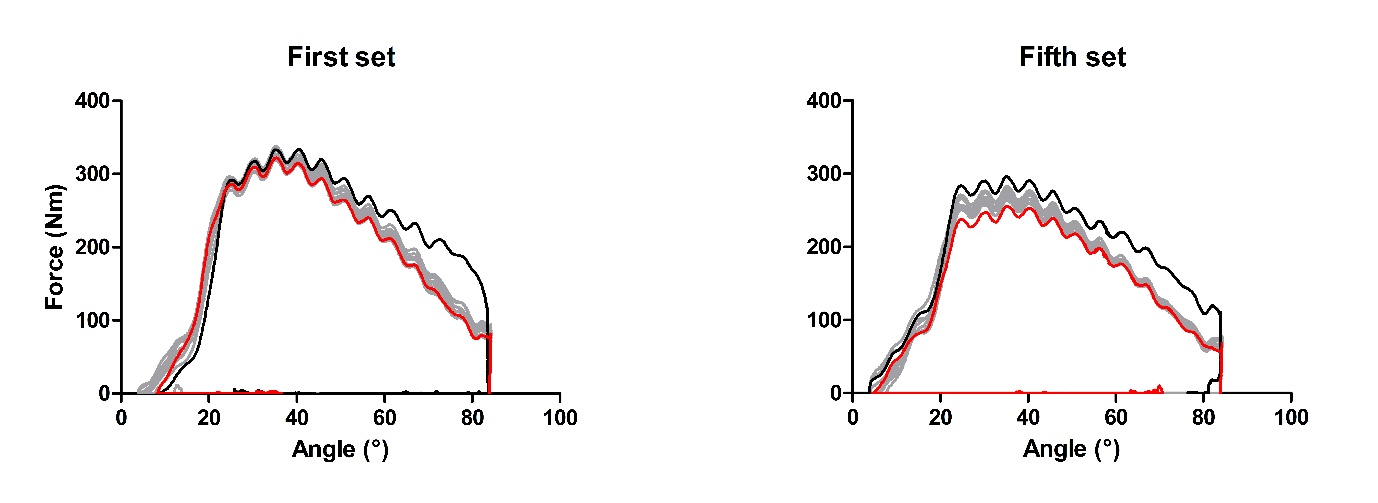
Figure 2 - Representative force traces from the twelfth training session of one participant. The higher force traces stem from the first contraction in each set (black line), the last repetition is represented in red. Stimulation intensity was 200 mA. The x-axis represents the knee angle with zero being full extension, force is measured in Nm, with positive values signifying eccentric force. The y-axis cut-off value is set to zero.
Ultrasound
Ultrasound was used to measure thigh composition including muscle thickness, as a proxy for muscle volume, and epidermal/lipid layers (Abe et al., 2015). Each participant was scanned thrice pre and post intervention at 25, 50 and 75% of thigh length, measured from the ilium to the superior prominence of the patella. The participant was placed in the dynamometer using the same settings as for testing and training. The leg was extended to 0 degrees (0 degrees being fully extended) and held by the dynamometers lever arm to allow the participant to relax the musculature. The participant was instructed to relax and sit still during all scans. During scanning, great care was taken not to compress the musculature and to measure in the same position every time. The ultrasound pictures were analysed offline using ImageJ (Schneider et al., 2012) by two different assessors to ensure reliability. The ultrasound apparatus used allowed for saving multiple pictures of each scan, which helped in taking uniform pictures (HS-2100, Honda electronics, Japan). Averages of all scans in each person are presented except for one participant, where the medial scan was very different between pre and post, here, the analysis omitted the medial scans, for the scan results, see appendix.
Data analysis
All figures are created using R-software (R version 4.3.0; R Development Core Team, 2022) or GraphPad Prism (Version 5.0.3; GraphPad Software, Massachusets USA GraphPad Prism). The R-code, dependencies and accompanying data is available online (https://doi.org/10.5281/zenodo.15495070; Gravholt et al., 2025). Due to the early cessation of the study, related to discomfort and adverse effects, no statistical tests were conducted. Rather, results from pre and post tests are presented as means ± SD and the mean difference [CI] when data was normally distributed (dynamic MVC and muscle thickness) to allow for future power calculations with the caveat that the study is underpowered (Arain et al., 2010). Data will be presented graphically and in tables as individual data points plus boxplots or average per training session ± SD.
Results
Feasibility
In 7 of 11 enrolled participants, the entire training protocol was completed. Four participants dropped out of the training intervention, all prior to the pre-test (three following the first familiarization, one following the second) session; one due to knee pain from an old injury, one from illness unrelated to the project, and two who stopped responding to communications. Among the completers, the training intensity was reduced for a week in one participant following complaints about knee pain, similarly, one participants stimulation intensity was increased at a slower rate than planned due to slight knee discomfort. Subsequently, the stimulation intensity could be increased again, similar to the remaining participants. Data on muscle soreness and stimulation related discomfort during training was not systematically noted, however, it was mentioned by several participants, although none that warranted changes to the protocol. Following the termination of the seventh participant, the study was forcibly stopped due to a countrywide covid-19 lockdown. Despite not having reached the intended inclusion number, it was decided at this point not to restart the study in light of the above-mentioned drop-outs and preliminary results showing minimal efficacy.
The training program showed notable increases in electrically evoked torque over the training period, this was on average 56 ± 22 % [34.6 : 77.1] of MVC torque (112 mA) during the first training session and increased to 101 ± 17 % [85.3 : 116:3] of MVC (204 mA) in the 12th and last training session. The change in electrically evoked torque and stimulation current is depicted in Figure 3.
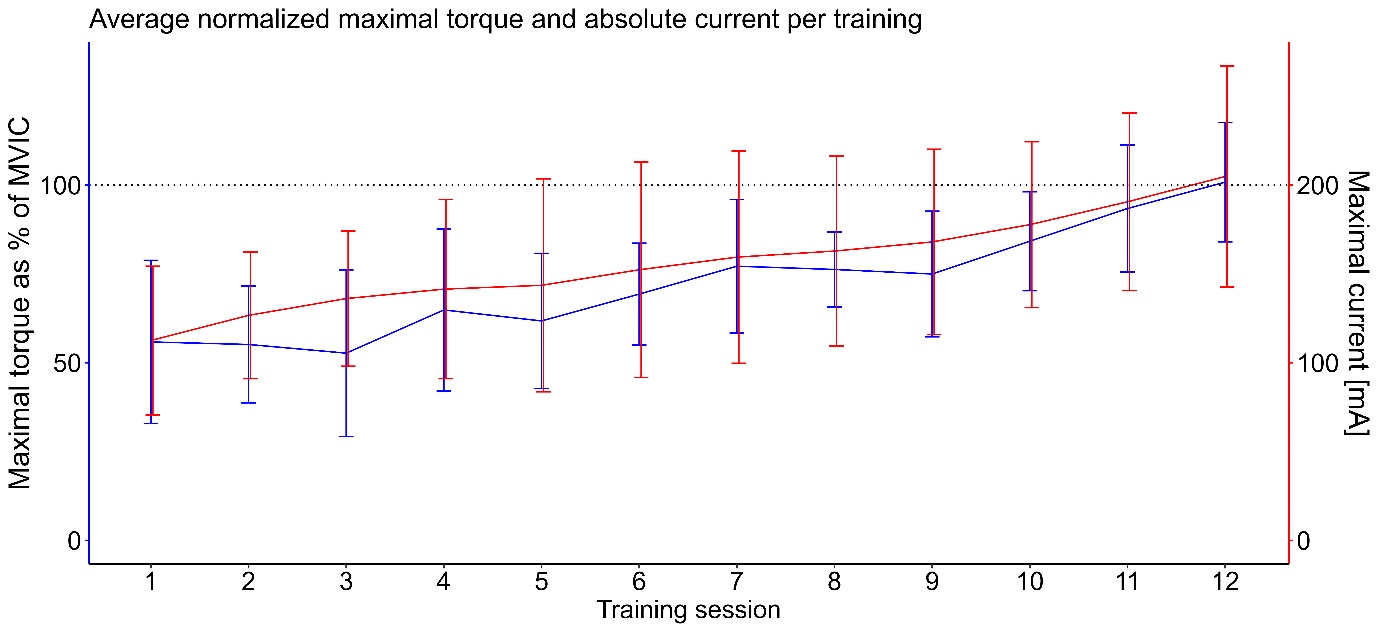
Figure 3 - Average values for maximal torque normalized to MVC and maximal current used in each training session. Torque (in blue) is presented as a percentage of the pre-test MVC ± SD whereas intensity (in red) is presented in mA ± SD with the other parameters being constant.
Outcome measures
Maximal voluntary isometric contractions for familiarization day one and two as well as pre and post data are presented in Figure 4A. Mean MVIC was: Pre: 278 ± 116 Nm, Post: 282 ± 116 Nm.
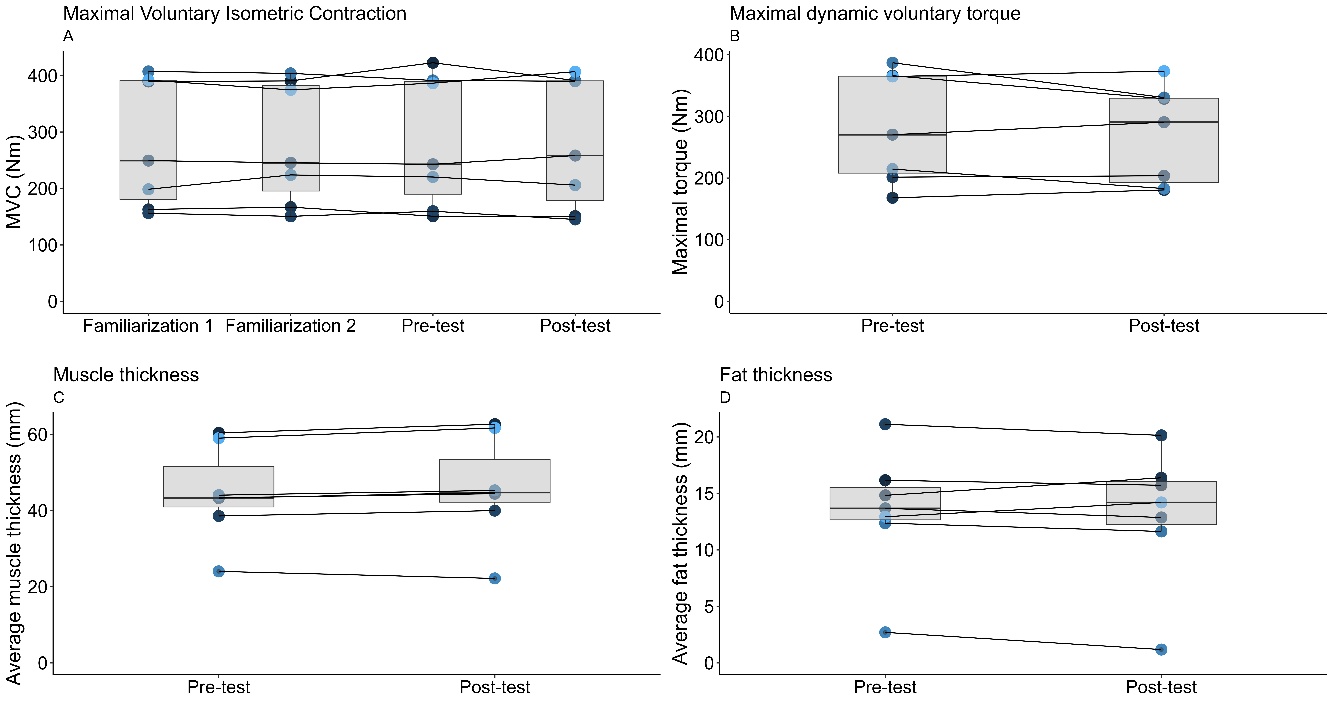
Figure 4 - A) Measures of maximal voluntary isometric contraction force for each participant. B) Change from pre to post in maximal voluntary dynamic contraction torque measured during the fatiguing protocol. The values depicted are the maximal torque values measured during the fatiguing task which was comprised of concentric and eccentric contractions at a constant velocity of 60 degrees / sec (15-90 degrees of knee flexion). All maximal torque values were obtained during the eccentric phase.C) Muscle and D) fat layer thickness before and after four weeks of training. Each colour represents a participant, the same colour is used for participants throughout. Notice that the y-axes are differently scaled.
Similar to MVIC, values in dynamic voluntary torque were relatively stable (Pre: 270 ± 79 Nm, Post: 282 ± 90 Nm, Post - Pre difference 11.68 [-15.7;39.1]) as depicted in Figure 4B.
By use of ultrasound, pre and post values were observed in muscle thickness (Pre: 44.3 mm ± 13.0, Post: 45.9 mm ± 13.5, Post - Pre difference 1.6 [1;2.1]) and in fat (Pre: 13.4 mm ± 5.56, Post: 13.2 mm ± 5.93) thickness, as depicted in Figure 4C and D.
Discussion
This study investigated the feasibility of 12 sessions of unilateral electrically stimulated eccentric leg extension exercise over the course of 4 weeks. A total of n=7 healthy young participants completed the exercise regimen, before the study was terminated due to a number of adverse events and general discomfort related to the stimulation. The main findings were that electrical stimulation eccentric training provides attainment of high torque levels near MVIC but was not accepted or tolerated by all healthy young participants .
Feasibility is a major concern in the current study. Four participants withdrew after the first two familiarization sessions, but prior to the first training session. One of the dropouts was study-related in the form of knee pain during electrical stimulation, whereas another was due to non-study-related illness. Although the remaining two did not give a reason for dropping out, it may be speculated that the electrical stimulation during testing and associated discomfort played a role, indicating a need for a less intense introduction to such a stimulation protocol. The increase in stimulation intensity we employed during familiarization was quite rapid and a more tapered approach appears to be necessary when using electrical stimulation in untrained individuals. This can, for example, be seen in the slow gradual increase in tolerated current as controlled by participants. Of note, the n=7 participants who stayed in the study for the training sessions, were able to complete the entire planned program with only minor adjustments made to the progression of electrical stimulation during training. However, among the completers of the study, muscle pain and discomfort were reported. Taken together, the eccentric electrical stimulation training program applied in the present study was not well tolerated in a group of healthy young participants. Hence, such an approach is likely not feasible in patient populations in need of physical rehabilitation. With the experiences obtained in this study, we propose a very gentle introduction to NMES. The requirement in the current study of force-velocity profiling in the beginning might have caused drop-outs that could potentially have been avoided with a longer introduction to increasing stimulation intensities.
The eccentric mode of exercise employed in the present study resembles regimens which have yielded improvements in both strength and muscle volume when conducted as voluntary movements (Vikne et al., 2006; Roig et al., 2009). Importantly, eccentric training excels in eliciting high muscle tension and increasing muscle volume when compared to concentric training (Roig et al., 2009). Indeed, a single bout of intense eccentric exercise is particularly associated with a high degree of muscle damage and muscle soreness (Vissing et al., 2008), but also a repeated bout effect decreasing the degree of damage upon subsequent eccentric exercise (Friden et al., 1989; Lieber & Friden, 1993). In our study, it is possible that the high intensity electrical stimulation has contributed to muscle damage similarly to the observed effects by Crameri et al. (2007), who reported larger disruptions in the muscle fiber from electrically stimulated compared to voluntary contractions. Similarly, increased contraction speed appears linked to an increased severity of muscle damage (Chapman et al., 2006; Chapman et al., 2008; Ochi et al., 2010). Altogether, the lack of systematic changes in muscle strength suggests that the present training protocol does not lead to excessive muscle damage. Meanwhile, the lack of positive training adaptations may be due to the short intervention period or the non-voluntary activation.
The lack of strength gain could indicate a need for longer rest-periods between training sessions. Each training session was accompanied by a substantial decrease in torque from the first set to the last set (average loss of maximal torque: -14.2 %), indicating a fatiguing effect of the electrically stimulated eccentric contractions. A downside to electrical stimulation is the repeated stimulation and activation of the same motor units, potentially causing exacerbated fatigue in only a subset of muscle fibers in a muscle (Gregory & Bickel, 2005; Crameri et al., 2007). A plethora of studies have suggested that high-frequency electrical stimulation leads to premature fatigue in the musculature. Bigland-Ritchie et al. (1979) observed a pronounced fatigue response when using high-frequency electrical stimulation rather than low-frequency stimulation. Accordingly, Fuglevand and Keen (2003) found that muscle force production was better maintained when contractions were evoked by ‘physiological’ discharge rates (⁓30 Hz) compared to higher and more artificial ‘lab-based’ discharge rates (60 Hz). However, results from our recent study on discomfort and electrical stimulation parameters further supports the use of high frequency stimulation to achieve high mechanical tension at moderate discomfort levels (Gravholt et al., 2023). Another issue with eccentric contractions has been discomfort of the patella tendon and knee joint linked to high mechanical forces. As reported, some participants reported discomfort in the knee joint during training, although this could be alleviated when stimulation intensity was temporarily lowered during the training intervention. Thus, one should be careful when administering high torque eccentric contractions to unaccustomed populations. Whilst the eccentric training modality and increases in current intensity and torque were well tolerated by most participants in the present study, the intervention could have benefitted from a longer duration and slower progression in intensity, with loads more similar to the general recommendations for untrained populations (American College of Sports, 2009).
Ultrasound measures were used to investigate changes in thigh muscle thickness as a proxy measure of muscle mass. We observed indications of small increases in measures of muscle thickness over the study period. This finding could be interesting to explore further in a full scale trial. However, it is uncertain whether this difference in thickness stem from muscle growth or transient oedema. The scans reveal localized increases in muscle thickness with three participants increasing muscle predominantly in the mid-thigh section and the other predominantly at the proximal and distal scan sites (see appendix).
Due to limited resources, the current pilot study did not use a control group to follow any natural evolution of strength and muscle size. Further, the intervention was relatively short and training interventions targeting prime movers in locomotion amongst healthy young participants may require longer interventions to improve muscle function. With the low number of participants, we remain careful in interpreting the pre-post data as actual intervention based changes since the low statistical power could lead to spurrious claims and difficulty in replication.
In summary, high torque can be elicited through electrical stimulation which was applied here in a training intervention using only electrical stimulation to elicit eccentric contractions. However, the regimen used in the present study was not well tolerated as many participants experienced muscle pain and others dropped out prior to the training intervention. Potential clinically important increases in muscle strength or mass may require longer intervention periods. Future studies should re-design the electrical stimulation exercise and make it less intense initially (and thus with less discomfort), before moving to full scale trials to investigate whether this can lead to long-term adaptations in muscle volume and strength, possibly in patient populations who are unable to exercise voluntarily.
Practical applications
The use of electrical stimulation has gained traction with the many commercially available devices. Common practice is the use of isometric contractions during electrically stimulated training interventions, while voluntary training often consists of dynamic contractions. We aimed to study the feasibility and outcomes of a short-term electrical stimulation only training intervention using eccentric contractions. Our data presented here indicate that one should be careful in the early administration of high-intensity electrical stimulations, as the initial experience might deter the participant from future use of electrical stimulation. In studies that apply NMES, a longer familiarization period might be useful. The completers (7 of 11) of our study accepted high intensity (100 % of MVC) dynamic training using only electrical stimulation. In practical applications, practitioners should, thus, focus on a gradual increase in training stimuli. Since we did not test isometric or concentric training in the current investigation, we cannot argue for or against the addition of dynamic contractions in the training program.
Author contributions
Author contributions according to CRedIT recommendations: Conceptualization (AG,JH,LH and KO), Methodology (AG,JH,CK, LH and KO), Formal Analysis (Lead) (AG), Investigation (AG, JH, CK), Data Curation (AG, JH, CK), Writing – Original Draft (AG, JH, KO), Visualization (AG, JH, KO), Writing – Review & Editing (AG, JH, CK, LH and KO), Supervision (LH, KO), Project Administration (AG, JH, CK), Funding Acquisition (AG).
Acknowledgements
Preprint version 4 of this article has been peer-reviewed and recommended by Peer Community In Health and Movement Science (https://doi.org/10.24072/pci.healthmovsci.100192; Frère, 2025).
Funding
AG received funding to renumerate participants from Helga and Peter Kornings Fond (DC472123-004-117).
Conflict of interest disclosure
The authors declare they comply with the PCI rule of having no financial conflicts of interest.
Data, scripts, code, and supplementary information availability
Data and R scripts are available online (https://doi.org/10.5281/zenodo.15495070; Gravholt et al., 2025).
Appendix

Figure A1 - Electrode placement and instrumentation
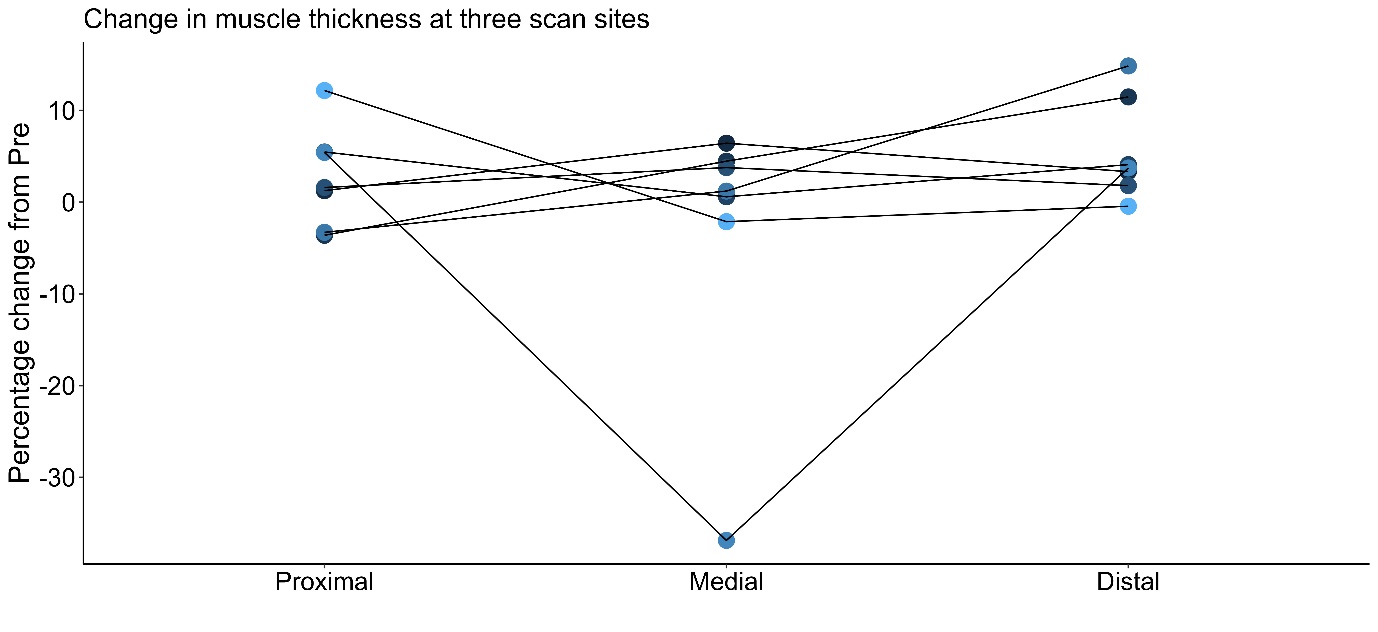
Figure A2 - Change in, proximal, medial and distal muscle thickness in percentage of pre-value. The outlier in the medial section appears to stem from a higher applied pressure during the scan and has been omitted in the statistical analyses of post-pre differences.