
 CC-BY 4.0
CC-BY 4.0
Introduction
Despite the importance of motivation in determining patient adherence to interventions and impact on treatment outcomes, little attention has been given to how motivational theory is being applied in physiotherapy practice. For physiotherapy interventions to be effective, a person must adhere to the proposed plan and complete the exercises suggested. Adherence to physiotherapy home exercise and management strategies throughout the duration of physiotherapy sessions is integral to short-term recovery, while long-term adherence can often reduce the incidence of recurrence or re-injury. Several intervention parameters such as duration, mode of delivery, cost, as well as behavioural factors including self-efficacy may influence adherence (Wu et al., 2025). Beyond the context of an intervention or behaviour of a client, a therapist’s behaviour may also have a significant impact on adherence. Precisely, interpersonal relationships, therapeutic relationship, shared-decision making are components that should be considered by a physiotherapist as they impact overall health outcome (Rodríguez-Nogueira et al., 2025). How a person behaves, in this case a physiotherapist, greatly influence motivation. Therapeutic relationships include person-centered care, interpersonal communication, and motivation strategies (Rodríguez-Nogueira et al., 2025) all components well reflected in the self-determination theory of motivation. According to the self-determination theory (SDT), interpersonal interactions are an integral part of the human experience that can directly influence the quality of the motivation of a targeted person, in this case a patient.
Self-Determination Theory
SDT is a broad and comprehensive motivational theory developed by Deci and Ryan that has been widely used in psychology to inform interventions in the education, management, and health care sectors (Ng et al., 2012; Ryan & Deci, 2000). According to SDT, motivation varies not only in function of quantity but also quality (Pelletier & Rocchi, 2023). That is, motivation is not a simple dichotomous construct where a person is more or less motivated to engage in a behavior, motivation can take different forms that vary according to their level of autonomy or self-determination. SDT typically distinguishes between autonomous and controlled motivations (Pelletier & Rocchi, 2023; Ryan & Deci, 2020). Autonomous motivation refers to behavior that could be intrinsically motivated (a behavior done because it is pleasurable, that is an end in itself) and to behavior that could be extrinsically motivated (i.e., a mean to an end) but still self-determined. SDT refers to two types of self-determined extrinsic motivation, integrated regulation (where a behavior is further internalized by taking in consideration other dimensions of the self that are considered important) and identified regulation (where an internalized behavior is done by choice because it is considered important). Controlled motivation refers to behavior that are regulated by internal factors (like internal obligations, shame, guilt) that have been poorly internalized or external factors (like incentives, constraints, pressures from others). The more a behavior is autonomously regulated (or self-determined), as opposed to controlled (or non self-determined), it is likely to be integrated to a lifestyle and to lead to positive outcomes such as well-being (Pelletier & Rocchi, 2023; Ryan & Deci, 2020).
SDT proposes that for a person to be fully autonomous motivated and engaged in an activity, therapists should support the development of autonomous motivation from a self-determination stance by fulfilling basic psychological needs of : (1) autonomy (i.e., the need for individuals to act in line with their own interests and values), (2) competence (i.e., opportunities for increasingly challenging activities and developing greater levels of mastery), and (3) relatedness (i.e., needing a caring, supportive social network with strong interpersonal connections) (Ryan & Deci, 2000, 2017). These three needs are said to be innate and universal across cultures. Need-supportive behaviours (i.e., supporting one’s autonomy, competence, and need for relatedness) promote need-supportive environments; while need-thwarting behaviours (autonomy thwarting/controlling, competence thwarting, and relatedness thwarting) lead to need-thwarting environments (Ryan & Deci, 2017). According to SDT, if an individual’s context supports their basic psychological needs, their needs are more likely to be satisfied, which leads to autonomous motivation for a given activity. This allows them to engage in that activity out of interest or curiosity, or because it is in line with their goals and objectives (Ryan & Deci, 2017). Alternatively, if an individual’s basic psychological needs are not met, they are more likely to be dissatisfied and engage in a behaviour for controlled reasons, such as to comply with or please someone else, or to avoid feeling guilt or shame. When individual engage in a behavior for controlled reasons, they are less likely to learn, to find the experience satisfying, and, in turn, to persist or maintain an activity. Since physiotherapy is often dependent on clients’ motivation and capacity for undergoing significant health behaviour change, a comprehensive review of how SDT improve patients’ active involvement with physiotherapy and facilitate health behavior change was necessary.
SDT in physiotherapy
Autonomous motivation has been identified as an important contributor to physical activity adoption and intervention adherence (Ntoumanis et al., 2021; Teixeira et al., 2012) and can enhance a patient’s active participation within medical encounters (Osei-Frimpong, 2017). In terms of healthcare service delivery, needs-supporting relationships are as important when delivering services in-person as when using telehealth (Ryan & Deci, 2000, 2017). Behaviours change techniques based on supporting basic psychological needs (autonomy, competence, relatedness) may present as goal setting, shared decision making, or occupational coaching in rehabilitation delivery. However, in rehabilitation-specific professions, the use of SDT is still in its infancy. In speech language pathology, a scoping review looking at aphasia and motivation identified a potential positive influence in clinical research for aphasia (Biel et al., 2022). In physiotherapy, the perception of a physiotherapist’s behaviour was shown to be important in the delivery of a telerehabilitation intervention (O’Neil et al., 2023a). Autonomy, competence, and relatedness-supporting strategies, including, but not limited to, sharing of achievements, encouragement, and exchange of information, were systematically highlighted to be critical in peer support pain management rehabilitation groups (Stenberg et al., 2022). Although the influence of SDT has been indirectly studied in areas related to physical activity adherence, pain reduction, return to sport, and aphasia interventions, a gap still exist in understanding its specific use in physiotherapy intervention and how SDT is being delivered in that specific context (Gillison et al., 2019; Ntoumanis et al., 2021).
According to the Canadian Physiotherapy Association, physiotherapy is “the assessment, diagnosis, and treatment of the human body, its diseases, disorders and conditions associated with physical function, and acute or chronic injury or pain. It includes the prevention of illness or injury and promotion and education on health and wellness with a focus on optimal movement and function” (Canadian Physiotherapy Association, 2024). Since prior physiotherapy research identified possible impact of components of self-determination theory implementation in a physiotherapy intervention (O’Neil et al., 2023a), we chose to document the precise use of this specific theory on the physiotherapy profession to facilitate reproducibility in a physiotherapy clinical context. In doing so, our aim is to examine the specific components of physiotherapy intervention that could be related to the satisfaction of the three basic needs proposed by SDT, that the behavior targeted by the intervention shows signs of internalization, and that this behavior is associated to the positive outcomes typically pursued by an effective physiotherapy intervention.
More specifically, the primary objective of this rapid review was to identify the physiotherapy contexts in which SDT is currently being used to determine whether using SDT principles within physiotherapy practice is effective at improving physiotherapy intervention adherence, facilitating education, and self-management. Our secondary objective was to describe the populations receiving SDT-based physiotherapy and how SDT-based physiotherapy interventions are being measured. Identifying this information will lead to the development of more effective SDT-driven physiotherapy interventions.
Methods
Rapid reviews improve accessibility and clarity of research evidence (Featherstone et al., 2015; Haby et al., 2016). Adhering to Cochrane methodology for rapid review (Garritty et al., 2021), we examined how SDT approaches are being used within physiotherapy services to inform future program development. Based on high-quality evidence (i.e., RCTs and SRs), we wanted to identify the clinical application of theory to the population being targeted by this type of intervention and the methods of delivery in a physiotherapy context. We registered our protocol in the Open Science Framework repository before starting data extraction (https://doi.org/10.17605/OSF.IO/FP8JM). Specifics of the Cochrane methodology for rapid review are described in each methodology section.
Search strategy
The search strategy was piloted in one database (i.e., MEDLINE) using Boolean logic “and/or” to combine specific MeSH terminology including study design (i.e., randomized controlled trial, systematic review), SDT (i.e., autonomy, determination, satisfaction, psychological needs, autonomous motivation), and physiotherapy (i.e., physical therapy, physiotherapy modalities, physical rehabilitation) (table in appendix). We subsequently expanded the search to include needs satisfaction in Cochrane Library (OVID), PsycInfo, and Embase databases between 1990 and January 2023. We updated the search in September 2024. We then hand searched the references of included full texts.
Study selection
We screened citations using the review management software CovidenceTM. Two reviewers (JO, JvI) piloted a standardized title and abstract form for calibration before screening all articles by using the same 30 studies found in the initial MEDLINE search. As per Cochrane rapid review methodology, after duplicates were removed, two reviewers independently screened 50% of the titles and abstracts based on the following inclusion and exclusion criteria: systematic reviews and RCTs published in English and studies targeting physiotherapy services or exercise interventions based on SDT. Exclusion criteria will be incomplete studies, poster or protocols. In this review, the person who delivered the exercise program or physical activity was considered. Precisely, to be included, for an exercise program to be considered a physiotherapy intervention, the intervention needed to be delivered by a physiotherapist. Exercise or physical activity interventions were excluded when they were delivered by other health professionals or when the provider was not specified.
Once consensus was achieved, one reviewer (JO) completed the review of all titles and abstracts. Our inclusion criteria were SRs and RCTs published in English between 1990-2024, targeting physiotherapy services (i.e., evaluation, interventions, service delivery) or exercise interventions provided by a physiotherapist, and used SDT in the development of the interventions or assessments. Protocols and observational studies were excluded. Using the same process as above, we screened 10 full-text studies to pilot the full-text reviewing form. One reviewer (JO) completed the screening of all full texts while another reviewer (JvI) independently screened all excluded full text. Conflicts were resolved by discussion between reviewers until consensus was reached.
Data extraction and synthesis
Data extraction was completed using a standardized form (appendix B) to extract how physiotherapy interventions and SDT techniques (i.e., communication, education, training program, behaviours, were delivered (i.e., in-person, telerehabilitation, hybrid), types of physiotherapy outcomes (i.e., adherence, effectiveness, health-equity) and SDT psychological needs(i.e., autonomy, competence, relatedness motivation, adherence, effectiveness, health-equity) being targeted, and the population and types of health conditions being investigated. The behavioural change technique classification of the data was informed by Teixeira et al. (2020). Data was extracted by one reviewer (initials here-anonymous) and reviewed by a second (initials here-anonymous). Two independent reviewers assessed Risk of Bias using the ROB2 tool (Sterne et al., 2019) for RCTs and the AMSTAR2 tool (Page et al., 2021; Shea et al., 2017). We followed the PRISMA reporting guidelines (Page et al., 2021). Findings were analyzed narratively following the review objectives to identify similarities and differences between studies and synthesized descriptively in tables (Dobbins, 2017).
Results
Included studies
Of 184 citations identified, we removed 58 duplicates, screened 126 titles and abstracts, reviewed 54 full-texts, and included 8 RCTs (n= 445 participants) and 1 SR (n=712 participants) (Figure 1). Interrater reliability for titles and abstracts selection was strong (k 0.88). The 9 studies retained in this review represented 1157 participants with an average age ranging from 3 to 77 years old. Only one systematic review targeted people under the age of 18 (Meyns et al., 2018). The terminology for sex and gender was often interchanged, leaving no explicit reporting of gender in any of the studies. The four most recent RCTs (Chair et al., 2024; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Wallbank et al., 2022) published between 2022 and 2024 reported more health equity indicators (i.e., socio-economic factors, employment, level of education, gender, race, and culture) compared to the four published earlier.
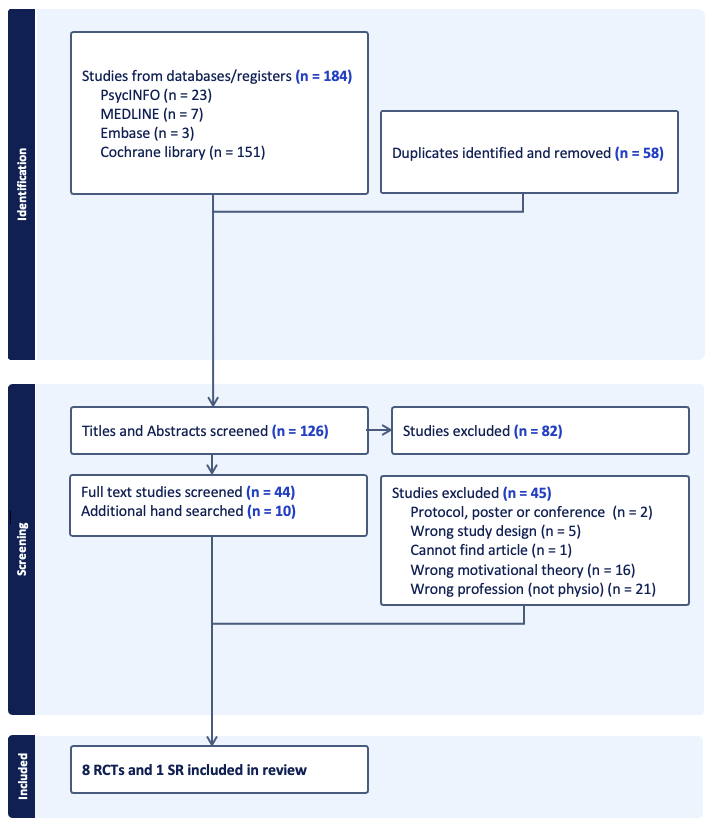
Figure 1 - Prisma Chart illustrating the identification, screening, and inclusion process (Page et al., 2021).
Risk of Bias
Overall, two of the RCTs were rated as low ROB while 6 RCTs were rated as having some concerns (Figure 2). Concerns were mostly related to the randomization process and missing data. The SR by was assessed as high quality using the AMSTAR 2 tool (Shea et al., 2017), however, the lack of protocol registration could introduce bias.

Figure 2 - Reporting on Risk of Bias (ROB) of the RCTs assessed by the ROB2 tool (Sterne et al., 2019).
Physiotherapy and SDT interventions
Patient populations included adults living with specific orthopedic conditions (including chronic low back pain, those requiring hip and knee replacements, and sedentary women) and adults and children with specific neurological conditions (including HIV, Huntington disease, and children with motor development conditions such as cerebral palsy, brachial plexus injuries, and gait development impairments, and autism spectrum disorder). One RCT targeted adults with coronary heart disorder and one was conducted with healthy students (Table 1).
Several types of physiotherapy interventions for children and adults were included such as traditional strength and aerobic exercise programs (Aunger et al., 2020; Chair et al., 2024; Hovland et al., 2013; Murray et al., 2015; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Shah et al., 2016), virtual reality therapy (Levac et al., 2017; Meyns et al., 2018), and equine-assisted therapy (Meyns et al., 2018). Diverse settings included outpatient hospitals (Aunger et al., 2020; Murray et al., 2015), hybrid interventions (Chair et al., 2024), home and community (Aunger et al., 2020; Chair et al., 2024; Meyns et al., 2018; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Shah et al., 2016; Wallbank et al., 2022) and research laboratories (Levac et al., 2017) (Table 1).
The SR by Meyns et al. focused on delivery of different motivational techniques including the use of virtual reality, robotics, circus-themed games in a goal-based approach to improve intrinsic motivation in children with developmental disorders (Meyns et al., 2018). Five out of eight RCTs used multifactorial motivational strategies including goal setting, education on physical activity, exploration of barriers and facilitators, problem solving, adherence, social interaction, and self-monitoring (Aunger et al., 2020; Chair et al., 2024; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Wallbank et al., 2022). Another RCT (Levac et al., 2017) conducted with healthy students in laboratory environments used virtual reality to compare autonomy-supportive and autonomy-controlling tasks. In contrast, Murray et al. (2015) used hybrid behavioural change techniques and methods of delivery, including video recording, vignettes, active role-playing, and group discussions to enhance the physiotherapist’s abilities to support their patient’s needs. Novel combinations of in-person, group videoconference, and phone applications (Nunez-Gaunaurd & Tovin, 2024), the benefit of music and phone calls (Chair et al., 2024), and phone interviewing and text-messages (Wallbank et al., 2022) were also documented. While other RCTs relied on a combination of simple methods, including in-person and phone calls (Quinn et al., 2022; Shah et al., 2016), Aunger et al. (2020) only included in-home, in-person motivational strategies (Aunger et al., 2020)(Table 2).
Outcomes and outcome measures
RCTs measured outcomes related to physical activity and function, behaviour changes, mental health outcomes, quality of life, and a combination of these (Table 3). Specific to physical activity level, seven RCTs (Aunger et al., 2020; Chair et al., 2024; Levac et al., 2017; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Shah et al., 2016; Wallbank et al., 2022) used a variety of outcome measures, including self-reported questionnaires, clinical assessment, and objective kinematic measures. Five RCTs (Aunger et al., 2020; Chair et al., 2024; Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022; Wallbank et al., 2022) used wearable technology to capture step count and overall daily physical activity in real-world context. Other physical outcomes and outcome measures included strength measured by dynamometer (Shah et al., 2016), function measured by daily repetitions of sit-to-stand (Aunger et al., 2020), and overall disability (Wallbank et al., 2022).
Outcomes related to needs-supportive behaviour changes and mental health were mostly measured using questionnaires and validated scales. Motivation and engagement were measured in the SR (Meyns et al., 2018) and six RCTs (Aunger et al., 2020; Chair et al., 2024; Levac et al., 2017; Nunez-Gaunaurd & Tovin, 2024; Shah et al., 2016; Wallbank et al., 2022). The most frequently used measure for motivation and engagement was the Behavioral Regulation in Exercise Questionnaire (3 out 9 studies). Changes in mood and mental health were measured in three RCTs (Quinn et al., 2022; Shah et al., 2016; Wallbank et al., 2022) with the Beck Depression Inventory, and the Positive and Negative Affect Schedule. Finally, quality of life was measured in three RCTs (Quinn et al., 2022; Shah et al., 2016; Wallbank et al., 2022) using three different measures, the Short-Form Health Survey-36, the Short-Form Health Survey-12, and the EuroQuol EQ-5D-5L survey.
Adherence or attendance was measured differently across studies, including reporting of adherence to action plans in a booklet (comprised of six goals and three environmental modifications) (Aunger et al., 2020) and percentage of sessions attended (Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022). Intervention fidelity was measured in 3 RCTs by rating the delivery of skills (Aunger et al., 2020), self-reporting checklist from physiotherapists (Quinn et al., 2022), and use of wearable sensors (Nunez-Gaunaurd & Tovin, 2024; Quinn et al., 2022). Two RCTs measured safety, and one RCT measured satisfaction and acceptability.
Efficacy of physiotherapy services combined with SDT interventions
One RCT reported a significant increase in physiotherapists’ needs-supportive behaviours with SDT interventions measured by the Health Care Climate Questionnaire (intervention arm [mean ±SD] = 4.6±0.85; control arm [mean ±SD] = 2.78 ±0.72) (Murray et al., 2015). In terms of intervention feasibility and acceptability, one RCT reported that combining in-person physiotherapy services with motivational interviewing, emotional support, education, and problem-solving is feasible and may have an impact on sedentariness in older adults awaiting hip and knee arthroplasty (Aunger et al., 2020). Another RCT demonstrated that combining online physiotherapy program with health coaching emails and text message was feasible and an acceptable for women over 50 years old (Wallbank et al., 2022). A third RCT showed that combining moderate-vigorous exercise 3–5 times per week with 18 physical activity coaching sessions may have a positive impact on walking endurance and self-reported physical activity in people living with Huntington’s disease (Quinn et al., 2022). Findings also suggest that combined physiotherapy interventions with SDT-based interventions could significantly improve physical function such as gait speed in people with HIV (Shah et al., 2016), exercise capacity and exercise efficacy in people with coronary heart disease (Chair et al., 2024), and self-reported physical activity in adults with autism spectrum disorder (Nunez-Gaunaurd & Tovin, 2024).
Table 1 - Physiotherapy interventions, intervention delivery, and outcomes. Abbreviations: HIV, human immunodeficiency virus; RCT, randomized controlled trial; SDT, self-determination theory.
|
Author, year, and sample size |
Physiotherapy interventions |
Intervention outcomes (i.e., adherence, engagement effectiveness, health-equity) |
Mode of delivery |
|---|---|---|---|
|
Systematic Review (N=1) including 3 RCT, 6 Case-control, 6 non-comparative studies |
|||
|
Systematic review |
Various physiotherapy interventions including virtual reality based therapy to train balance and strength (8 studies), Modified constraint-induced therapy (1 study), supported treadmill training (1 study), Robotic (1 study), circus-camp (1 study) for children with developmental disorders. Parameters ranged from 1 day 12 minutes session to 20 weeks |
Compliance: VR is an innovative or fun aspect to increase the participants’ exercise time or compliance (12 studies). Physical Activity: exergames did not provide as vigorous physical activity training as the physical fitness exercises (1study) |
Various modes of delivery including in-person, virtual reality, robot-assisted |
|
Randomized controlled trials (RCTs) (n=8) |
|||
|
Randomized controlled trials (n=48) |
Communication skill training for physiotherapist working with adults with chronic back pain |
No outcome on patients |
In-person physiotherapy delivery in outpatient clinics |
|
Randomized controlled trials (n=67) |
Individually tailored 12-weeks community-based physical activity program that included walking at moderate intensity and 10 tailored, moderate to intense resistance strength training exercises for upper and lower body ranging from 1-4 set of 8-15 repetitions with exercise training bands. Adults with HIV-infected at risk of functional decline |
Physical activity: Significant improvements in physical function and activity within the treatment group. Depression: Significant improvement in emotional well-being and role limitations due to physical health in the treatment group compared to the control group |
Recommended by an experienced physical therapist |
|
Randomized controlled trials (n=40) |
No physiotherapy intervention for patient provided |
Engagement: Participants in the autonomy-supportive group demonstrated better retention (i.e. shorter movement time) on sequence. There were no significant differences between groups in overall or subscale user engagement scale. |
Virtual reality delivered in a research laboratory |
|
Randomized controlled trials (n=35) |
Physiotherapy intervention for older adults waiting for hip or knee replacement surgery |
Adherence: 88% completion rate Physical activity: Eight (42.1%) achieved or exceeded their step targets, usual care (4907 mean steps per day) vs intervention group (5170 mean steps per day) |
In-person physiotherapy delivery |
|
Randomized controlled trials |
The Active Women over 50 Online Program offered over 3-months in the community |
Acceptability: 83% participants would recommend participation to another person |
Online program offered in the community |
|
Randomized controlled trials (n=57) |
The PACE-HD is a physical activity program that includes 18 sessions of 30-minutes of moderate-vigorous exercise, 3–5 times per week for adults living with Huntington’s disease |
Adherence: 80.5% adherence Physical activity: Differences walking endurance and self-reported PA at 12 months favoring the intervention group |
In-person or videoconference by a physiotherapist |
|
Chair et al. 2024 (n =130) |
An 8-week hybrid program including 16 supervised center-based exercise sessions (2 hours/session, 2 sessions/week) of prescribed exercises and home-based self-paced program for adults living with coronary heart disease |
Exercise capacity: The intervention group demonstrated statistically significantly greater improvements in exercise capacity compared to control group |
Hybrid program |
|
Randomized controlled trials (n = 18) |
A 12-week intervention including aerobic and strengthening exercises once a week with progressions during week 3 to 10 for adults between 18 and 32 years of age with a diagnosis of autism spectrum disorder |
Adherence: Attendance to weekly telehealth sessions ranged from 70 to 100%, with a mean of 93%. Wearable adherence ranged from 20 to 100%, with a mean of 82%. Physical Activity: Significant effect from the intervention for physical activity pre-post-test and based on steps/day |
Telehealth-synchronous program |
Table 2 - Motivation Behaviour Change Techniques (MBCT), SDT intervention and delivery and outcomes. Abbreviations: MBCT - Motivation Behaviour Change Techniques, SDT – Self-determination theory. Note: The number beside MBCT refers to the Classification of Motivation and Behavior Change Techniques label/taxonomy.
|
Author, year, and sample size |
Motivation Behaviour Change Techniques (MBCT) and SDT interventions |
Outcomes |
Mode of delivery |
|---|---|---|---|
|
Systematic Review |
12 out of 15 studies included fun aspects targeting intrinsic motivation. This included VR games for motivation for motor rehabilitation (5 studies) |
Intrinsic motivation: The authors found that exergames initially had a high intrinsic motivational power with high situational interest that attracted the children (lasting effects of Challenge, Exploration and Instant Enjoyment). This indicates that a diversion from the exercise (movie) provides a similarly increased motivation to “go through” with the rehabilitation as being immersed in the VR game to increase the intrinsic motivation actively participate in the rehabilitation |
Virtual reality as mode of delivery |
|
Randomized controlled trials (n=48) |
1. Competence-support techniques MBCT 18. Offer constructive, clear, and relevant feedback. |
Needs-supportive behaviours: A large difference in needs-support scores between physiotherapist in intervention group physiotherapists rated as significantly more supportive than control arm physiotherapists |
Hybrid delivery using videorecording, vignettes, active role-playing, and group discussion |
|
Randomized controlled trials (n=67) |
1. Autonomy supportive interventions MBCT 6. Provide choice 2. Competence-support techniques |
Intrinsic motivation: No clear evidence of treatment effects on, perceived competence, or intrinsic regulation, however, participants who improved in intrinsic motivation also improved in gait speed |
60 minute in-person counseling session and telephone counseling sessions |
|
Randomized controlled trials (n=40) |
1. Autonomy supportive interventions |
Intrinsic motivation: There was a significant difference between groups in overall IMI score with the autonomy supportive group performing higher on overall motivation |
In a research laboratory |
|
Randomized controlled trials (n=35) |
1. Competence-support techniques 2. Relatedness-support techniques |
No specific behaviour change outcomes reported |
Delivered in 2 visits in the person’s home |
|
Randomized controlled trials |
1. Relatedness-support techniques |
Acceptability: 87% participants chose to receive motivational messages, 79% opened email messages sent, 31% of the embedded links were clicked on, and 88% of participants indicated the telephone health coaching session supported their PA |
Emails and SMS messages (as per patient preference) delivered via telephone by a tertiary-qualified physiotherapist trained in motivational interviewing |
|
Randomized controlled trials |
1. Autonomy supportive interventions 2. Competence-support techniques |
Acceptability: Participants reported a very high level of satisfaction with 20/20 (100%) agreeing or strongly agreeing that they were satisfied by and enjoyed the therapist-led sessions. |
Delivered on the phone by a site coordinators or licensed physical therapists |
|
Randomized controlled trials |
Autonomy supportive interventions MBCT 4. Explore life aspirations and values |
Self-efficacy: The intervention group had significantly improved exercise self-efficacy compared to control group |
In-person and telephone-based |
|
Randomized controlled trials |
1. Competence-support techniques 2. Relatedness-support techniques |
Relatedness, competence, and autonomy supportive |
Weekly individual and group online discussion for 10 weeks |
Table 3 - Outcomes measures used in physical or behaviour change domains. Abbreviations: EuroQol EQ-5D-5L, European Quality of Life – 5 Dimensions, 5 Levels; ISWT, Incremental Shuttle Walk Test; PA, physical activity; WHO, World Health Organization
|
References, date |
Physical outcomes and outcome measures |
Behaviour changes, mental health outcomes, and outcome measures |
Intervention feasibility and fidelity outcomes and outcome measures |
|---|---|---|---|
|
Systematic Review |
|||
|
Not applicable |
Motivation and engagement: Pediatric Volitional Questionnaire, Pediatric Motivational Scale, Children’s Assessment of Participation and Enjoyment, Situational Interest Scale-Elementary school, Family Participation |
Satisfaction: Likert scale assessing fun in rehabilitation |
|
|
Randomized Controlled Trials |
|||
|
Not applicable |
Needs-supportive behaviours: Health Care Climate Questionnaire |
Not applicable |
|
|
Physical function and physical activity: Physical Performance Test, a MicroFET 2; time needed to complete an obstacle course; six-minute walk test; gait speed; 12-item Physical Activities Scale for the Elderly questionnaire; Paffenburger Physical Activity Index Physical function (strength): hand-held dynamometer |
Motivation and engagement: 3-item Locus of Causality for PA scale; Behavioral Regulation in Exercise Questionnaire-2; Perceived Competence scale is a 4-item scale Mental health: the Beck Depression Inventory-II Quality of life: the Short-Form Health Survey-36 |
Not applicable |
|
|
Physical function: Acquisition and Retention time |
Motivation and engagement: Intrinsic Motivation Inventory; User Engagement Scale |
Not applicable |
|
|
Physical activity levels: ActivPal3 to measure sedentary time, steps per day, measure of Older Adults Sedentary Time, Short Physical Performance Battery Physical function (strength): daily sit-to-stand |
Motivation and needs supportive behaviours: Basic Psychology Needs Scale |
Adherence and compliance: adherence to action plan in booklet Intervention fidelity: rating of delivery skills (support of basic psychological needs, motivational interview, problem solving, progress monitoring, setback management) |
|
|
Physical activity levels: average number of daily steps measured by ActiGraph GT3X+ accelerometer; self-reported physical activity, measured by the International Physical Activity Questionnaire; proportion of participants meeting at least the lower limits of the WHO physical activity guidelines; 150 min/week of moderate-intensity physical activity or 75 min/week of vigorous-intensity physical activity or an equivalent combination of both, measured by ActiGraph GT3X+ accelerometer Physical function: function component of the Late Life Function and Disability Instrument |
Motivation and Exercise efficacy: Exercise perceptions, measured by the Exercise Benefits and Barriers Scale Mental health and mood: the Positive and Negative Affect Schedule Health-related quality of life: EuroQol EQ-5D-5L survey |
Acceptability: whether participants would recommend study participation to another person |
|
|
Physical activity levels: wearable activity monitors (Fitbit Charge 2) to monitor PA (e.g. step counts, activity intensity and frequency). |
Mental health and behaviour: Short Problem Behavior Assessment, Hospital Anxiety and Depression Scale combined with the Snaith Irritability Scale Health-related quality of life: Short-Form Health Survey (SF-12) |
Adherence: % of sessions attended Intervention fidelity: therapist self-report checklists completed after each session and therapist self-assessment rating scale; average number of days participants had Fitbit devices and % of days with valid wear time (defined as ≥10 h) Safety: calculating the number of adverse events and number of falls in intervention and control groups |
|
|
Physical Activity Levels: the 10-m ISWT; heart rate using a sensor (Polar H7, Polar Electol GmbH, Germany); blood pressure and heart rate before and after the test; perceived exertion at the beginning and end of the test; accelerometer for 7 days; the validated International Physical Activity Questionnaire-Short Form |
Exercise self-efficacy and self-determination: the validated Chinese version of the Cardiac Exercise Self-Efficacy Instrument; Behavioural Regulation in Exercise Questionnaire |
Not applicable |
|
|
Physical activity levels: Godin-Shephard Leisure-Time Physical Activity Questionnaire, Fitbit Inspire (Fitbit® Inc., San Francisco, California, USA), for 10-weeks. Adiposity Anthropometric assessments: body mass index; waist to height ratio via telehealth |
Exercise self-determination: Behavioral Regulation in Scale; relative autonomy index |
Adherence: attendance to session Intervention fidelity: wearable adherence Safety: adverse events related to music-paced physical activity |
|
Discussion
In this rapid review, we describe the use of SDT techniques combined with physiotherapy interventions, how they are measured, and their reported outcomes based on high quality evidence. Our findings also provide some insight on how physiotherapy interventions combined with SDT techniques are currently being delivered (e.g., aerobic exercise, virtual reality, problem-solving tools, reframing), how are these interventions currently being assessed (e.g., physical activity levels, motivation, mood and behaviour), and for whom they have been designed. Overall, our findings suggest that SDT techniques combined directly with specific physiotherapy interventions is feasible for people with a variety of health conditions, including children with neurodevelopmental disorders such as cerebral palsy, adults with certain neurological conditions including HIV and Huntington’s disease, adults waiting hip or knee replacement or who are sedentary, and adults with cardiovascular conditions. Studies on the impact of physiotherapy and SDT interventions developed for adults and older adults with neurological conditions such as stroke, traumatic brain injury, spinal cord injury, and neuroinflammatory conditions are still lacking (Kors et al., 2022; Sawatsky et al., 2022). Since research shows that personalization and tailoring of physiotherapy interventions based on the SDT framework positively impact motivation in people who have experienced a stroke (Sivertsen et al., 2022), however the current literature does not report enough details on the types of tailoring or motivational strategies to enable clinical recommendations or replication (McEwen et al., 2019) . It is necessary to understand the specific motivation and behaviour change techniques used within specific contexts and with specific populations to tailor care.
This review also showed that supporting competence of physiotherapist using SDT techniques may indirectly influence communication skills of physiotherapists, which may improve therapeutic relationships between clinicians and patients (O’Neil et al., 2023a). Furthermore, results from cohort studies included in Meyns et al. suggest that the use of virtual reality as well as meaningful partnerships may improve active engagement within a physiotherapy and effectiveness of the intervention (Bilde et al., 2011; Brütsch et al., 2011; Harris & Reid, 2005; Järvikoski et al., 2015). The impacts of combining SDT specific behaviour change techniques within a physiotherapy framework may have an impact on both, clinicians and patients. Consistent with findings from a meta-analysis by McGrance et al., motivational SDT interventions included in this rapid intervention primarily improved adherence, exercise behaviour, and levels of physical activity (McGrane et al., 2015). From a motivational and behaviour change perspective, results from this rapid review also showed positive outcomes related to clinicians’ needs supportive behaviours as well as patients’ self-efficacy and acceptance. The challenges now lie with knowledge of such complex interventions and how to implement them clinically. Approaches such as co-creation of interventions or shared-decision activities might be beneficial (Osei-Frimpong, 2017) . Training of future physiotherapist on the implementation of behaviour change within a clinical context is critical.
Furthermore, our results suggest that is feasible for physiotherapy interventions combined with behaviour changes and SDT techniques to be delivered in various modes. It demonstrates the potential of alternative physiotherapy delivery options (i.e., in-person, telerehabilitation, robot-assisted, hybrid) and SDT techniques delivery options (e.g., in-person, telerehabilitation, virtual reality, phone sessions, text-messages). When comparing in-person and telerehabilitation in physiotherapy, emerging evidence shows similar results for satisfaction, adherence, and effectiveness for certain conditions (Kloek et al., 2018; Lara-Palomo et al., 2022; Seron et al., 2021). Our findings showcase the acceptability and effectiveness of diverse physiotherapy care delivery. Similarly, the delivery of interventions, both physiotherapy and SDT, was reported to be feasible and accepted in various settings (hospital, virtual reality, research laboratory, vignettes). Further high-quality research is needed to explore how physiotherapy and behaviour change techniques can be integrated in complex interventions, to identify if the method of delivery has an impact on outcome, and how the method of delivery may influence the design of complex telerehabilitation interventions.
Interesting findings around outcome measures is highlighted. Our rapid review demonstrated a lack of standardized outcome measures related to autonomous motivation, communication and interpersonal behaviours and their validation for physiotherapy interventions. This is an important clinical and research gap since autonomous motivation has been demonstrated to have an impact on health behaviour (Sheeran et al., 2021). Assessment tools objectively measuring the impact of SDT combined with physiotherapy interventions may be necessary to demonstrate the effectiveness of SDT-driven physiotherapy. Reliance of self-report may create limitation in the assessment of effectiveness of SDT-driven physiotherapy. Rouse et al. provide an example of a validated tool measuring the interpersonal support in physical activity consultation (Rouse et al., 2016). Others have proposed self-determination specific questionnaires such as the Health Care Climate Questionnaire, the Perceived Competence Scale, and Treatment Self-Regulation Questionnaire. Without access to or use of validated tools designed to measure if and how a motivation-based intervention may influence physiotherapy interventions, the inclusion of SDT interventions within physiotherapy may be limited. This review could influence the development or clinical use of new self-determination-based outcome measures that are simple to use in all geographical context and languages.
Finally, demographic findings demonstrate gaps in explicit reporting of health equity indicators. Reporting of health equity indicators could not only improve transparency in reporting but provide critical information on the context in which the person is living (O’Neill et al., 2014) for whom a combined physiotherapy and SDT intervention would be beneficial. Results from our updated search demonstrates a positive trend in the reporting of key socio-demographic indicators. Future work should document in detail how health equity indicators are considered and how SDT interventions and supporting basic psychological needs could influence the effectiveness of an intervention from a sex and gender-based analysis, a cost-effectiveness analysis, or an accessibility analysis.
Practical Implications
-
Supporting basic psychological needs combined with physiotherapy interventions may have a positive impact on a clinician’s therapeutic approach as well as certain patient health outcomes, adherence to intervention, and the development of effective therapeutic relationships. Behaviour change techniques should be systematically included as part of the physiotherapy curriculum as well as a continuing education topic for current physiotherapists, focusing on hands-on implementation rather than theoretical ideas .
-
Combining physiotherapy interventions and SDT techniques is feasible and acceptable for various health conditions within various health care settings. It is therefore important to document how these interventions have been implemented and integrated into new interventions or clinical practice to facilitate implementation.
-
Combining physiotherapy interventions (i.e., moderate to high intensity resistance training, aerobic training, constraint–induced movement therapy) and SDT techniques (virtual reality, person-centered coaching sessions, music) can improve adherence to intervention, physical activity levels, and intrinsic motivation. Physiotherapists should strive to combine these interventions tools to improve self-efficacy and consequently efficacy of interventions.
Limitations
We acknowledge that the exclusion of other motivational theories may limit the generalization of our results. Future reviews may want to include other motivational theories, compare their impact, and synthesize their differences. It is critical to consider some limitations encountered during the screening and selection process of the studies. Unfortunately, the type of provider delivering the physical activity, physiotherapy of exercise program was often not reported. Since “physiotherapy or physiotherapist” was a specific inclusion criterion, many studies discussing ‘health or rehabilitation’ interventions were excluded. There is a need to report who is providing the intervention in studies to enable replication as well as personalize training around SDT for each health profession. The SDT interventions and behavioural change techniques presented in this review were not always reported based on the target behaviour change (competence, autonomy, relatedness support). Similar to documenting the details of physiotherapy interventions, precise reporting using validated measures of autonomous motivation or precise reporting of how the basic psychological needs of competence, autonomy, and relatedness may be supported or thwarted in physiotherapy, could impact clinical practice and effectiveness of physiotherapy interventions (Ng et al., 2012). Furthermore, due to the lack of consistency in outcome measures, a meta-analysis of results was not possible for this rapid review. It is therefore essential to consider using consistent validated measures, such as validated measures of physiotherapist’s needs-supportive and needs-thwarting interpersonal behaviours, and autonomous and controlled motivation for engaging in physiotherapy, when conducting effectiveness trials to allow for the development of robust clinical guidelines on SDT driven physiotherapy interventions. To mitigate this limitation, we narratively synthesized the results from each included study which allowed us to provide preliminary information on feasibility and effectiveness.
Conclusion
With a growing push towards the use of person-centered approaches, goal setting, and shared decision making in physiotherapy, results from this rapid review demonstrate how SDT-designed physiotherapy intervention can be clinically implemented by identifying various types of SDT and physiotherapy interventions across various contexts. This review also identified key SDT interventions such as problem solving, problem monitoring, and goal setting which may, when combined with evidence-based physiotherapy interventions, improve the effectiveness of interventions. However, given the paucity of evidence of SDT interventions within physiotherapy, further research around implementation and delivery is needed before robust conclusions can be drawn as to the effectiveness on patient outcomes. This information may facilitate clinical implementation of SDT within physiotherapy, provide guidelines for the initiation and maintenance of health behaviours and specific adherence-interventions, as well as inform future training of physiotherapists.
Appendices
Appendix A: Search Strategies
|
Study design |
Self-determination theory |
Physiotherapy |
|---|---|---|
|
Medline (Ovid) randomized controlled trial (RCT): “randomized controlled trial”[Publication Type] OR “randomized controlled trials as topic”[MeSH Terms] OR “randomized controlled trial”[All Fields] OR “randomised controlled trial”[All Fields] systematic reviews: “systematic review”[Publication Type] OR “systematic reviews as topic”[MeSH Terms] OR “systematic reviews”[All Fields] |
Self-determination: “personal autonomy”[MeSH Terms] OR (“personal”[All Fields] AND “autonomy”[All Fields]) OR “personal autonomy”[All Fields] OR (“self”[All Fields] AND “determination”[All Fields]) OR “self-determination”[All Fields] theory: “theorie”[All Fields] OR “theories”[All Fields] OR “theory”[All Fields] OR “theory’s”[All Fields] Satisfaction of psychological needs or therapists’ interpersonal behavior |
physiotherapy: “physical therapy modalities”[MeSH Terms] OR (“physical”[All Fields] AND “therapy”[All Fields] AND “modalities”[All Fields]) OR “physical therapy modalities”[All Fields] OR “physiotherapies”[All Fields] OR “physiotherapy”[All Fields] physical therapy: “physical therapy modalities”[MeSH Terms] OR (“physical”[All Fields] AND “therapy”[All Fields] AND “modalities”[All Fields]) OR “physical therapy modalities”[All Fields] OR (“physical”[All Fields] AND “therapy”[All Fields]) OR “physical therapy”[All Fields] physical: “physical examination”[MeSH Terms] OR (“physical”[All Fields] AND “examination”[All Fields]) OR “physical examination”[All Fields] OR “physical”[All Fields] OR “physically”[All Fields] OR “physicals”[All Fields] rehabilitation: “rehabilitant”[All Fields] OR “rehabilitant’s”[All Fields] OR “rehabilitants”[All Fields] OR “rehabilitate”[All Fields] OR “rehabilitated”[All Fields] OR “rehabilitates”[All Fields] OR “rehabilitating”[All Fields] OR “rehabilitation”[MeSH Terms] OR “rehabilitation”[All Fields] OR “rehabilitations”[All Fields] OR “rehabilitative”[All Fields] OR “rehabilitation”[Subheading] OR “rehabilitation’s”[All Fields] OR “rehabilitation”[All Fields] OR “rehabilitator”[All Fields] OR “rehabilitators”[All Fields] |
|
Cochrane library (OVID) (systematic reviews or randomized controlled trial).af. |
(Self-determination theory or autonomous motivation).af. (Satisfaction of basic psychological needs or therapist interpersonal behavior) |
(Physiotherapy or physical therapy or physical rehabilitation).af. |
|
Psychinfo (OVID) (systematic reviews or randomized controlled trial or RCT).af. RCT or randomized controlled trials).mp. [mp=title, abstract, heading word, table of contents, key concepts, original title, tests & measures, mesh word] |
(Self-determination theory or autonomous motivation or SDT).af. or (Satisfaction of basic psychological needs or therapist interpersonal behavior) |
(Physiotherapy or Physical therapy or Physical rehabilitation).af. |
|
Embase (randomized controlled trials or RCT or Systematic reviews).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
(Self-determination theory or autonomous motivation or SDT).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] Or Satisfaction of basic psychological needs or therapist interpersonal behavior |
(Physiotherapy or Physical therapy or Physical rehabilitation).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
Appendix B: Data extraction form
|
Study and design general information |
Design Publication date Journal Authors and countries Sample size |
|---|---|
|
Objective 1: How physiotherapy services and SDT intervention were delivered |
Physiotherapy services in-person, telerehabilitation, hybrid Describe the type of delivery: SDT intervention in-person, telerehabilitation, hybrid Describe the type of delivery: |
|
Objective 2: WHY? types of outcomes being targeted |
Motivation types of motivation (e.g., autonomous, extrinsic...) Adherence how was it measured? Effectiveness how was it measured? health-equity how was it measured? |
|
Objective 3: WHO, the population and types of health conditions |
Population Age Sexe and or gender Culture? Other characteristics Health conditions |
Acknowledgements
Preprint version 3 of this article has been peer-reviewed and recommended by Peer Community In Health and Movement Sciences (https://doi.org/10.24072/pci.healthmovsci.100196; Bernard, 2026)
Data, scripts, code, and supplementary information availability
All data produced in the present study are made available on the OSF registration website (https://doi.org/10.17605/OSF.IO/JVPE3; O’Neil et al., 2023b).
Conflict of interest disclosure
The authors declare that they comply with the PCI rule of having no financial conflicts of interest in relation to the content of the article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.